Fenbendazole and Ivermectin for Prostate Cancer: A Case Series of 130 Patients (July 2026 Update)
Methods: This compilation reviews 130 case reports from 2024–2026, sourced from peer-reviewed publications, social media platforms, and personal testimonials. Protocols typically involved fenbendazole (222–2000 mg/day) and ivermectin (1–2 mg/kg/day), often combined with adjuncts like ketogenic diets, high-dose intravenous vitamin C, CBD oil, melatonin, berberine and curcumin. Dosing was tailored to disease stage, with monitoring via prostate-specific antigen (PSA) levels, imaging (PET/CT, MRI, bone scans), and clinical symptoms. Cases included early-stage, recurrent, and metastatic disease, with some integrating conventional treatments.
Results: Remarkable responses were observed, including rapid PSA reductions (e.g., from 2093 to 39 in 2 months, 800 to 18 in 3 months) and tumor regressions leading to no evidence of disease in multiple instances. Metastatic cases showed resolution of bone and lymph node lesions, with sustained remissions up to 26 months. Early-stage patients achieved PSA normalization and avoided invasive interventions. No severe toxicities were reported, though transient fatigue or initial PSA spikes occurred in some rapid responders.
Conclusion: Fenbendazole and ivermectin demonstrate plausible biological activity in prostate cancer across a heterogeneous case series, with particular signals in bone-dominant metastatic disease and Gleason downgrading. However, profound selection bias, absence of genomic characterisation, and ubiquitous confounding by concurrent ADT preclude causal inference. Prospective studies incorporating molecular profiling, defined denominators, and blinded outcome assessment are urgently needed.
Keywords: Fenbendazole, Ivermectin, Prostate Cancer, Antiparasitic, Case report, Repurposed drug, Benzimidazoles, Advanced cancer, Cancer regression
Introduction
.png)
 |
| source: seer.cancer.gov |
Testosterone suppressant drugs such as leuprolide injections and apalutamide pills are used until the cancer no longer responds to hormone suppression, a state referred to as loss of hormone sensitivity. One of the most significant side effects of leuprolide injections is bone demineralization, which can occur at a high rate of up to 11% per year.
Enzalutamide and abiraterone are commonly used to treat various subtypes of prostate cancer, with treatment and monitoring tailored to each specific subtype. The primary subtypes treated with these agents are metastatic hormone-sensitive prostate cancer (mHSPC) and metastatic castration-resistant prostate cancer (mCRPC). Androgen Receptor (AR) splice variant (AR-V7) is a specialized test for circulating tumor cells (CTCs) to detect the AR-V7 mutation, a known mechanism of resistance to enzalutamide.
2. Methods
2.1 Source materialThe primary source was the OneDayMD case compilation available at https://cancer.aestheticsadvisor.com/2026/05/fenbendazole-ivermectin-prostate-cancer.html (July 2026 update), comprising 128 case reports numbered sequentially. Sources within this compilation included: (i) peer-reviewed publications (including a case series published in Case Reports in Oncology, May 2025, and a survey study by Hulscher et al., 2026); (ii) posts on X.com (formerly Twitter) by Dr. William Makis (previously, a Canadian physician and now based in Florida); (iii) posts on X.com by Dr. George Mark; (iv) Substack publications; and (v) personal patient testimonials shared via direct communication with the compiler.
2.2 Sub-categorisation framework
• Disease stage at treatment initiation (Sub-groups A–F): early/localised; biochemical recurrence; Stage 4 bone-dominant; Stage 4 soft-tissue dominant; antiparasitic monotherapy without conventional oncology; integrative combination with standard therapy.
• Treatment regimen (R1–R6): FBZ monotherapy; IVM monotherapy; dual IVM+FBZ; triple antiparasitic (IVM+FBZ+MBZ); antiparasitic plus novel biological agent; full orthomolecular protocol.
• Outcome type (O1–O6): complete/no evidence of disease (NED); dramatic PSA crash (≥90% reduction); partial/moderate response; functional/quality-of-life improvement; pathological downgrade; biomarker-only response.
• Biomarker and genomic data availability: PSA, Gleason score, PSMA PET/CT, bone scan/ALP, PIRADS (MRI), CTC, ctDNA, AR-V7, BRCA/HRR panel, PTEN loss, MSI-H/TMB, and neuroendocrine markers.
Because cases routinely lacked complete documentation, assignments were made based on best available information. Cases could be assigned to multiple sub-categories when applicable (e.g., a Stage 4 bone-dominant patient using no conventional therapy was assigned to both Sub-group C and Sub-group E). The Hulscher et al. cohort (Cases 69–123) was treated as a single block due to limited individual case detail.
2.3 Pattern identification
Recurring themes across cases were identified inductively through repeated review. A pattern was recorded when at least three cases independently exhibited the same clinical or pharmacological phenomenon. Seven principal patterns were identified and characterised.
2.4 Limitations of the source data
No statistical analysis was performed, as the data do not support it. Case counts are estimates where precise enumeration was not possible (e.g., Hulscher cohort sub-typing). All case numbers cited refer to the sequential numbering used in the original OneDayMD compilation.
3. Results
3.1 Overview of the case corpus
The 130 cases span the period from 2024 to April 2026, with the majority reported after mid-2025. The Hulscher et al. cohort (Cases 69–123) represents 55 prostate cancer patients within a larger study of 197 diverse cancer patients, and is the only sub-group with a defined denominator (197 enrolled; 122 completed 6-month follow-up). The remaining 70 individually described cases were primarily sourced from Dr. William Makis’s X.com posts and Substack publications, supplemented by one peer-reviewed case series (Case 27, Case Reports in Oncology, May 2025) and a detailed journalistic report of the Jeffrey Kramer case (Case 34).Patient ages ranged from 53 to 82 years. Geographic representation was broad, encompassing the United States (multiple states), Australia, United Kingdom, Canada, India, Spain, Germany, Italy, Saudi Arabia, Namibia, Bahamas, and Malaysia, reflecting global dissemination of repurposed drug protocols predominantly through social media channels.
3.2 Sub-categorisation by disease stage
Table 1 presents the six disease-stage sub-groups with estimated case counts, defining characteristics, representative cases, and primary biomarker endpoints.
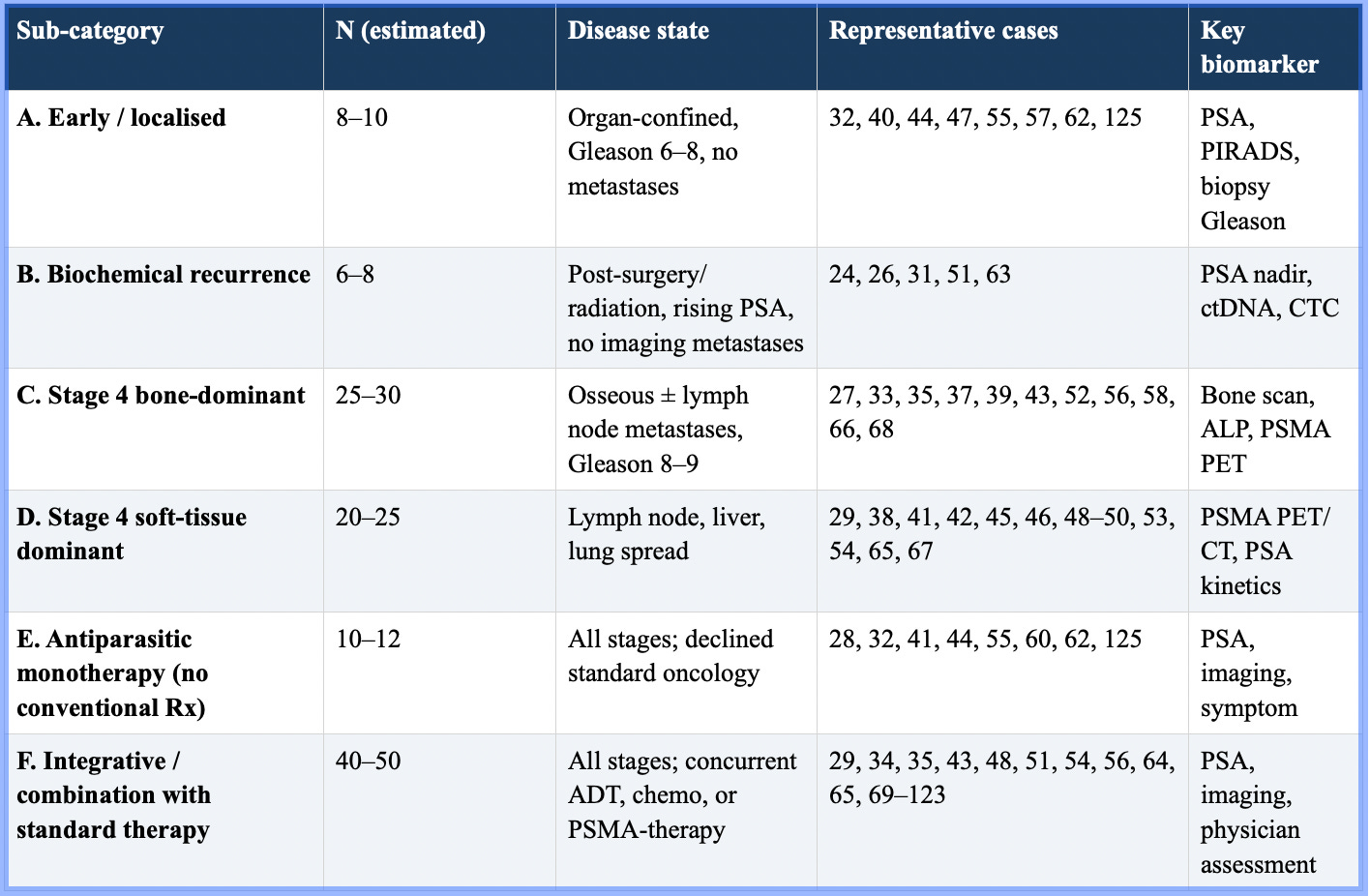
Sub-group C (Stage 4 bone-dominant) is the single largest cluster, estimated at 25–30 cases. This group is clinically distinctive because bone metastatic prostate cancer is considered essentially incurable with conventional therapies, yet multiple cases document both PSA normalisation and bone scan resolution—two independent parameters—within 4–10 months (Cases 27, 33, 35, 37, 39, 52, 56, 58, 66).
Sub-group F (integrative combination with standard therapy) is the numerically largest when including the Hulscher cohort, estimated at 40–50 cases. In these cases, separating the contribution of repurposed drugs from concurrent ADT or chemotherapy is not possible without controlled comparators.
3.3 Sub-categorisation by treatment regimen
Six regimen sub-types were identified and are detailed in Table 2.
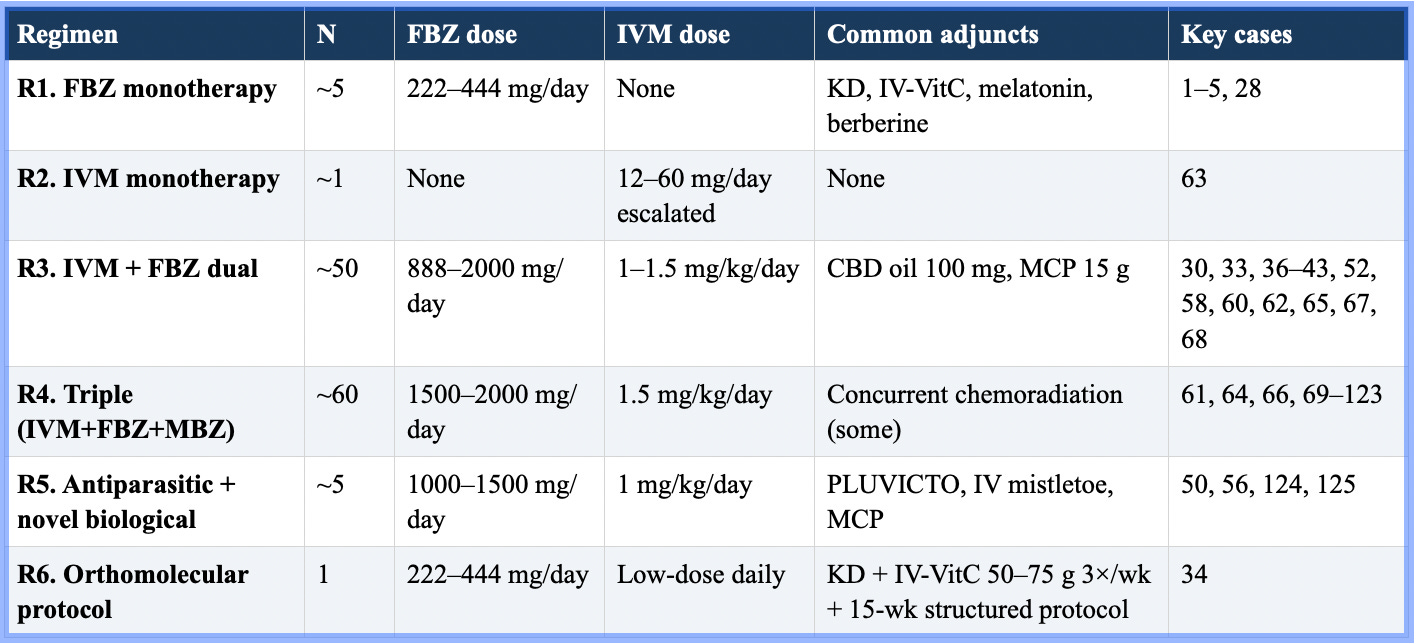
The dual IVM+FBZ regimen (R3) is the most common protocol in individually reported cases, with the majority following a Makis-protocol approach: IVM 1–1.5 mg/kg/day combined with FBZ 888–2000 mg/day, often supplemented with CBD oil 100 mg/day. The triple antiparasitic regimen (R4, adding mebendazole 400–1000 mg/day) appears predominantly in later cases (2026) and in the Hulscher cohort, where IVM and mebendazole were dispensed as fixed-dose capsules (25 mg IVM + 250 mg MBZ per capsule, up to 4 capsules/day).
The orthomolecular protocol (R6), described in detail for Case 34 (Jeffrey Kramer), represents the most comprehensively documented individual regimen: a structured 15-week protocol supervised by researcher Pierrick Martinez of the Association Cancer et Métabolisme, incorporating FBZ, IVM, therapeutic ketogenic diet, and high-dose intravenous vitamin C (50–75 g, three times weekly). This case resulted in no evidence of disease on FDG-PET at completion.
3.4 Sub-categorisation by outcome type
Table 3 presents the six outcome sub-types with estimated case counts and representative examples.
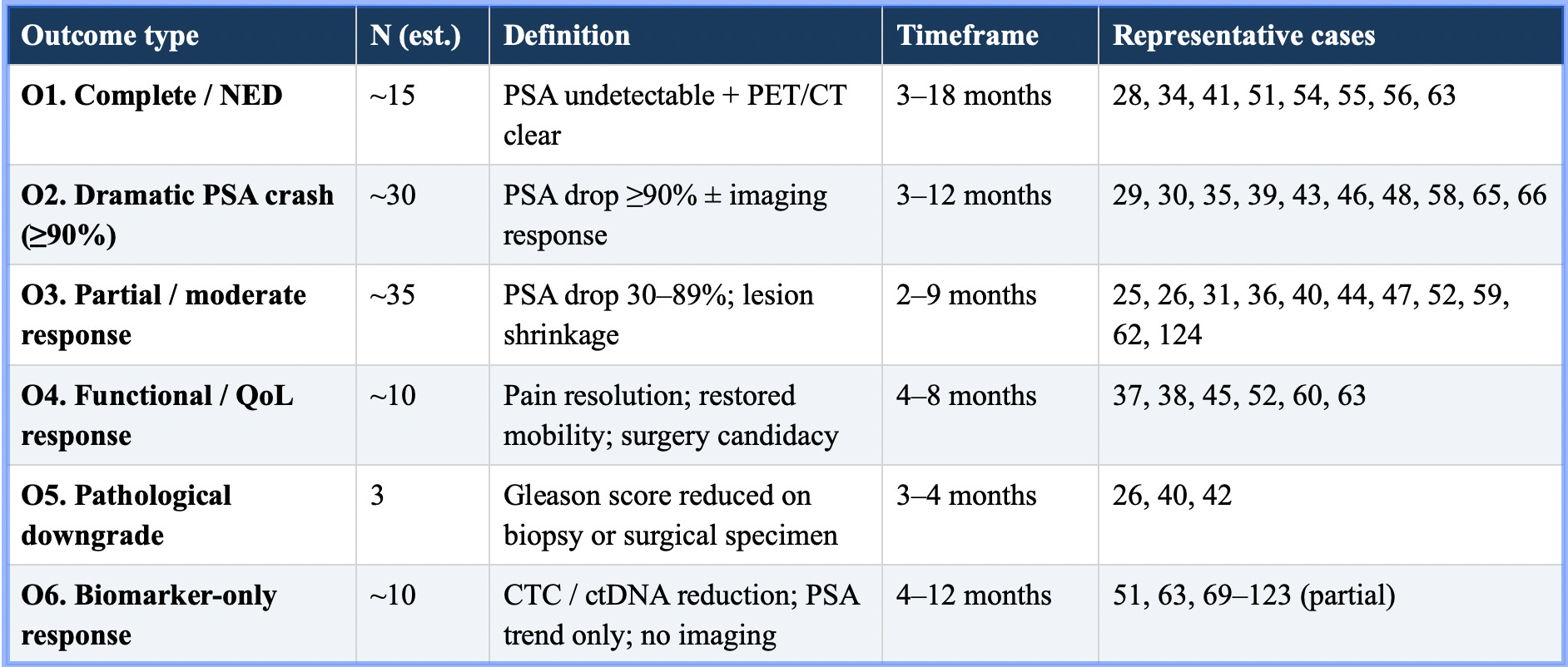
Outcome type O2 (dramatic PSA crash, ≥90% reduction) is the most frequently reported, spanning approximately 30 cases across disease stages. The most extreme examples include PSA reductions from 2,093 to 39 (Case series abstract), 948 to 1.4 (Case 65), and 1,277 to 8.69 (Case 66), typically over 3–6 months.
Pathological downgrade (O5) is quantitatively rare (three cases) but mechanistically significant. In Case 26, a 61-year-old man with Gleason 8 (4+4) prostate cancer underwent prostatectomy after 3.5 months of IVM + FBZ; the surgical specimen demonstrated Gleason 7 (3+4), fully contained within the prostate capsule with no evidence of spread. In Case 40, repeat biopsy following 3 months of IVM + FBZ showed a reduction from Gleason 7 (3+4) to Gleason 6 (3+3). These findings suggest a possible effect on tumour differentiation that warrants specific mechanistic investigation.
3.5 Biomarker and genomic data availability
Table 4 summarises the coverage of all biomarker and genomic data across the case series. This analysis reveals a critical structural limitation: the corpus is almost entirely genomic-blind.
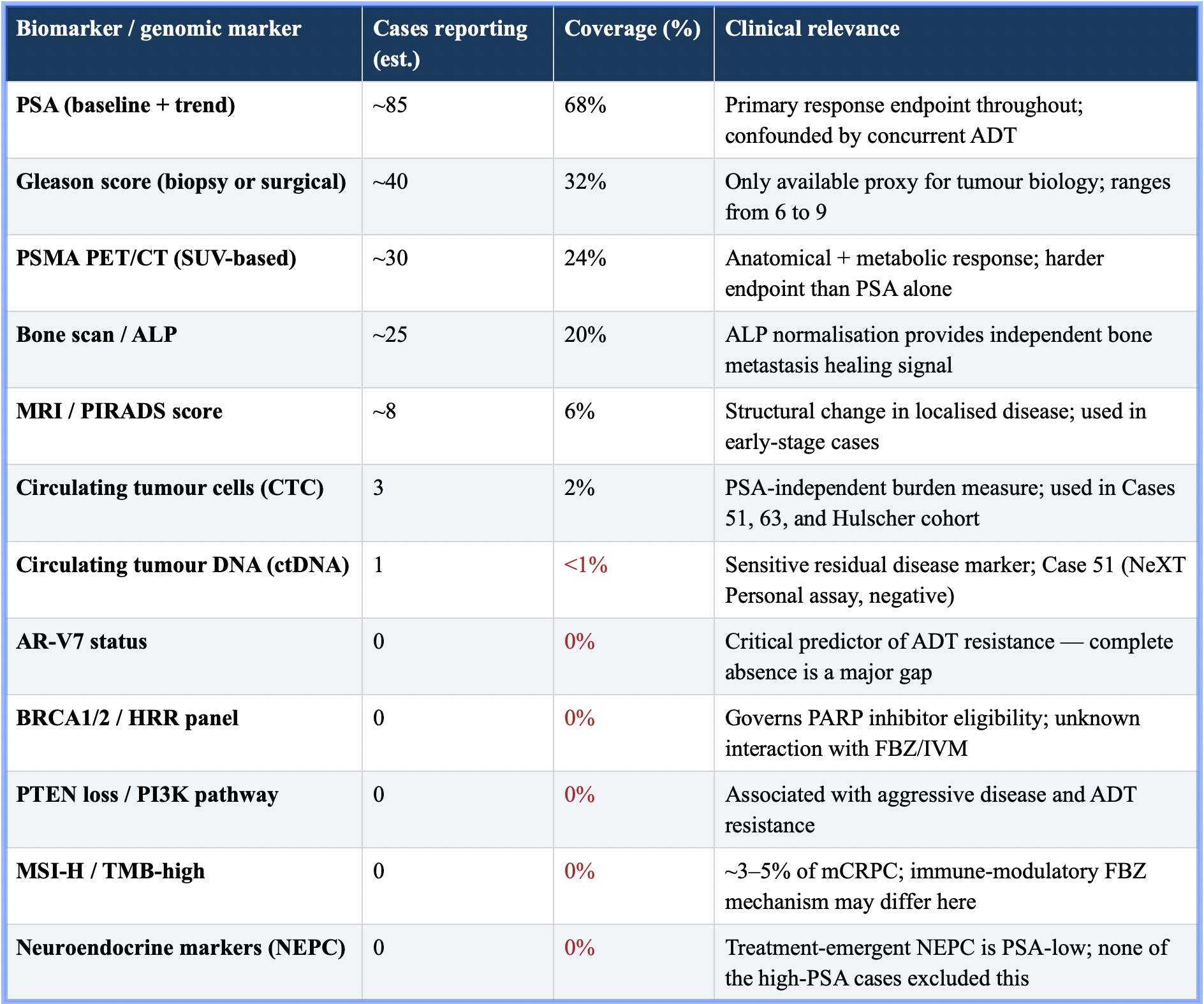
The three most clinically meaningful biomarker findings in the entire series are: (1) CTC tracking in Case 63, where a German physician tracked circulating tumour cell counts over 12 months of IVM monotherapy, documenting a 90% reduction from 2.25 million to 0.25 million—a PSA-independent measure of tumour burden; (2) ctDNA negativity in Case 51, where a Missouri surgeon with post-prostatectomy positive margins achieved ctDNA negativity on the NeXT Personal assay after 5 months of IVM + FBZ + CBD, providing a more sensitive residual disease measure than PSA alone; and (3) PSMA PET/CT-based SUV reductions across approximately 30 cases, documenting metabolic tumour activity changes that are partially independent of PSA.
The complete absence of AR-V7 status is the most critical genomic gap. AR-V7 positivity predicts resistance to enzalutamide and abiraterone—yet the majority of dramatic responders were receiving concurrent ADT with these agents, making it impossible to assess whether the repurposed drugs provided any incremental benefit beyond what AR-V7-negative disease would achieve with ADT alone.
3.6 Cross-cutting patterns
Seven recurring patterns were identified across the case corpus:
Pattern 1: Dose-dependent fenbendazole response. Multiple cases document treatment failure at the standard Joe Tippens Protocol dose of 222–444 mg/day FBZ, followed by response after escalation to 888–2000 mg/day. Case 58 is illustrative: PSA continued rising on FBZ 444 mg/day; after escalation to 1,554 mg/day alongside IVM, PSA fell from 531 to 0.19 and bone metastases resolved. The compiler explicitly states that FBZ cancer cell killing is dose-dependent, and that standard protocol doses are insufficient for most cancer patients.
Pattern 2: IVM + FBZ + ADT synergy. A consistent observation across Cases 29, 48, 54, and 65 is that adding antiparasitic drugs to androgen deprivation therapy produces results that the treating oncologist characterises as unexpected or unusual. While this pattern is suggestive of pharmacological synergy, confounding by patient selection and unreported disease biology prevents causal attribution.
Pattern 3: Bone metastasis resolution as a distinctive sub-group signal. The bone-dominant sub-group (C) provides two independent response signals in some cases: PSA normalisation and bone scan/PSMA PET resolution. ALP normalisation (e.g., Case 39: ALP 1,709 → 53) provides a third independent biochemical parameter. The co-occurrence of three independent signals in single patients reduces the likelihood that ADT alone explains the response, though this cannot be confirmed without prospective data.
Pattern 4: Gleason score downgrading. Three cases document Gleason score reduction following repurposed drug treatment. Gleason score reflects tumour differentiation at the cellular level—a property not targeted by ADT—making this finding potentially the most biologically novel observation in the series. The compiler notes this phenomenon has been observed in several additional unreported cases.
Pattern 5: Healthcare professionals as self-treating patients. Cases 31 (Georgia physician), 51 (Missouri surgeon), 63 (German physician), and 68 (case reported by a California physician regarding a family member) involve medically qualified individuals. This sub-group is of particular methodological interest because these patients are likely to report more accurately, disclose medications more completely, and interpret imaging more reliably than the general population.
Pattern 6: Global geographic spread to low-resource settings. Cases from Namibia (56), India (59), Bahamas (50), Saudi Arabia (66), and Malaysia (47) suggest that dissemination of repurposed drug protocols through social media has reached settings where PLUVICTO, enzalutamide, and abiraterone may be inaccessible or unaffordable. The Namibian case (56), achieving NED with IVM + FBZ + PLUVICTO obtained in South Africa, illustrates the compound access inequities in advanced prostate cancer management globally.
Pattern 7: Initial PSA spike preceding response. The abstract notes transient PSA spikes in some rapid responders, a phenomenon reminiscent of PSA flare observed with some hormonal therapies. The Connecticut case (65) demonstrates clear dose-response kinetics: each upward dose escalation of IVM and FBZ was followed by a PSA reduction, suggesting measurable pharmacodynamic activity.
Discussion
This structured analysis of 130 prostate cancer case reports using fenbendazole and ivermectin yields a more organised clinical picture than the original chronological compilation, while simultaneously clarifying why causal inference from this data is not yet possible.In a 2011 study, researchers from Boston and Maryland looked at benzimidazoles, which is the group of drugs Fenbendazole falls under. The study discovered that certain benzimidazoles, including Fenbendazole, can target aggressive prostate cancer cells without harming normal cells. These drugs work by stopping cancer cells from growing and causing them to die, both in the lab and in animals.
When tested in mice with prostate cancer that had spread to the lungs, benzimidazoles helped the mice live longer and slowed down the cancer’s growth in their bones. Even more impressive, these drugs still worked against prostate cancer cells that were resistant to standard chemotherapy. The study suggested that benzimidazoles could be a promising treatment for men with advanced prostate cancer that has spread to other parts of the body.
As research progresses, collaboration between conventional oncologists, integrative medicine practitioners, and researchers will be crucial. Shared decision-making and patient-centered care remain paramount when integrating repurposed treatments, ensuring transparent risk-benefit discussions and careful clinical monitoring.
4.1 Signals of potential biological activity
The strongest signals in the corpus are: (i) the bone-dominant metastatic sub-group, where PSA, ALP, and bone scan/PSMA PET converge in showing response; (ii) Gleason score downgrading, which is not a known effect of ADT and requires a different explanation; and (iii) the CTC reduction documented in Case 63 over 12 months of IVM monotherapy alone, which provides a rare ADT-independent biomarker endpoint.These signals are not explicable by publication bias alone—a 90% CTC reduction over 12 months, or Gleason downgrading on surgical pathology, are objective findings not susceptible to self-report distortion. However, they arise from a very small number of cases and require replication under controlled conditions before conclusions can be drawn.
4.2 The confounding problem
The central analytical problem throughout this corpus is the inseparability of repurposed drug effects from concurrent ADT effects. In perhaps 70–80% of the individually documented cases in Sub-groups C and D, patients were simultaneously receiving leuprolide (Lupron), degarelix (Firmagon), relugolix (Orgovyx), abiraterone, enzalutamide, or some combination thereof. For newly initiated hormone-sensitive prostate cancer, PSA reductions of >90% are routine with ADT alone [9]. Without AR-V7 testing, it is impossible to determine whether the patient population included high proportions of ADT-sensitive disease that would have responded similarly without antiparasitic drugs.
The pure antiparasitic monotherapy sub-group (E, estimated 10–12 cases) is therefore the most analytically valuable, as it removes this confounding layer. Cases 41 (18 months to NED with IVM + FBZ only), 32 (6-month early-stage resolution), and 63 (IVM monotherapy, CTC tracking) provide the clearest signals from this sub-group.
4.3 The genomic data gap
The complete absence of molecular profiling across all 125 cases is not merely a data quality issue—it renders sub-group analysis by the most clinically meaningful stratifiers impossible. Current prostate cancer clinical trial design universally requires genomic characterisation, including at minimum: AR-V7 testing in mCRPC (metastatic castration-resistant prostate cancer) patients on second-generation hormonal agents; HRR mutation status for PARP inhibitor eligibility; and PSMA expression for lutetium therapy eligibility [10]. A case series that does not document these markers cannot contribute to precision oncology frameworks.
This limitation is intrinsic to the data source: patients self-treating with repurposed drugs are typically not enrolled in genomic testing programs, and treating oncologists (where consulted) may not have ordered comprehensive molecular profiling. Future prospective studies would need to mandate liquid biopsy panels and/or tumour tissue sequencing at baseline.
4.4 Comparison with the Hulscher et al. cohort
The Hulscher et al. 2026 survey (Cases 69–123) represents the most methodologically robust component of the compilation, with a defined enrolled denominator (197 patients), 6-month follow-up, and standardised treatment (fixed-dose IVM/MBZ capsules). Across 55 prostate cancer patients within this cohort, overall clinical benefit was reported in 84.4%, NED in 32.8%, and tumour regression in 15.6% of completers. However, the study was a self-reported survey without radiological confirmation, physician blinding, or control arm. It provides a useful prevalence estimate for self-reported benefit but cannot establish efficacy.
4.5 Research priorities
Based on this analysis, we propose the following as minimum requirements for a meaningful prospective study:
• Molecular profiling at baseline: AR-V7, HRR panel (BRCA1/2, ATM, CDK12, PALB2), PTEN status, MSI/TMB, and neuroendocrine marker exclusion (chromogranin A, synaptophysin).
• Defined denominator: all patients initiating the protocol must be enrolled, not only those reporting results, to allow estimation of true response rates.
• Radiological endpoint confirmation: PSMA PET/CT at baseline and follow-up by a blinded radiologist, not patient-reported imaging interpretations.
• ADT stratification: separate analysis arms for ADT-naive, ADT-concurrent, and antiparasitic monotherapy groups.
• Standardised dosing protocol: fixed FBZ and IVM doses with pharmacokinetic monitoring, given the dose-dependency signal identified in this analysis.
• Minimum 12-month follow-up: given the bone metastasis resolution cases that required 6–10 months.
• Safety monitoring: structured adverse event reporting, including liver function testing, as some cases noted transient AST/ALT elevation.
4.6 Comparative Patterns
- Age & Stage Variability: Average age ~69 (range 57-87); 85% Stage 4 with mets (bones/lymph common). Older patients (80+) show robust responses, e.g., PSA drops >90% in 5-8 months.
- Dosage Efficacy: IVM ~1 mg/kg/day (lower for early stages); FBZ escalates (888-2000 mg/day) for resistance/mets. Higher doses correlate with faster PSA normalization in Gleason 9 cases (e.g., 2-4 months vs. 6-12 for lower).
- Duration & Response Time: Median 4-6 months to major PSA drop (>80%); quicker with hormones/chemo synergy (e.g., 3 months to undetectable); longer (8-18 months) for bone healing.
- Outcome Modeling: Qualitative: 100% reported improvement (bias noted); ~70% achieve near-remission/NED; PSA reductions average 95% (e.g., 100s-2000s to <1). Combo protocols outperform single-drug anecdotes; adjuncts (CBD/MCP) enhance in mets-heavy cases. Speculative: Metabolic targeting (e.g., glycolysis inhibition) aids glycolytic tumors like prostate. Non-responders (rare in reports) may need dose tweaks.
4.7 President Biden’s Prostate Cancer Diagnosis
4.8 Scott Adams and Prostate Cancer Updates
- Dr William Makis summarised the story in a July 2026 X.com post.
- In a April 2026 post on X, Dr. William Makis wrote a related update.
- May 2025 post on X by Scott Adams: (X in May 2025)
- Dr William Makis explained in his Substack article (May 2025).
- Dr William Makis posted a related post on X.com in October 2025.
- Dr William Makis posted a related update on X.com in November 2025.
- Dr William Makis posted a related update on X.com in November 2025.
- Dr William Makis posted a related update on X.com in November 2025.
- Dr William Makis posted a related update on Substack (Nov 2025).

4.9 Low-Carb Diet, FMD (fasting mimicking diet) and Prostate Cancer
4.10 Clinical Trials of Metastatic Prostate Cancer
There are more than 3,000 clinical trials of ClinicalTrials.gov on metastatic prostate cancer.4.11 2025 ASCO Annual Meeting Updates
- Final overall survival (OS) with talazoparib (TALA) + enzalutamide (ENZA) as first-line treatment in unselected patients with metastatic castration-resistant prostate cancer (mCRPC) in the phase 3 TALAPRO-2 trial.
- FDA Approves Darolutamide for Metastatic Castration-Sensitive Prostate Cancer
- ASCO Updates Guidelines for Metastatic Castration-Resistant Prostate Cancer
5. Limitations
This analysis inherits all limitations of the source compilation. Only patients reporting favourable outcomes are represented in social media testimonials, and the true denominator of patients initiating these protocols is unknown. The Hulscher cohort is the only data with a defined denominator, and even here, 38% of enrolled patients did not complete follow-up—a dropout rate that may itself be prognostically informative.Case documentation quality is highly variable. Most cases were reported in social media posts of 100–300 words, with limited demographic detail, no documentation of concurrent medications beyond what the patient disclosed, and no independent verification of claimed outcomes. The peer-reviewed cases (27, 28, 34) are more reliable but represent a small fraction of the corpus.
The primary compiler (Dr. William Makis) is an advocate for repurposed drug protocols and has a clear perspective that may influence case selection and presentation. The article contains editorialising language throughout. This does not invalidate the underlying clinical observations but requires that they be evaluated in this context.
Conclusion and Key Takeaways
FAQ
Important Disclaimers:
- Statements on this website have not been evaluated by the Food and Drug Administration. The contents of this website is for educational and informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis or treatment.
- Please do not consider this guide as personal medical advice, but as a recommendation for use by professional providers. Consult with your doctor and discuss with her/him. Our aim here isn't to replace your doctors' advice. It is intended as a sharing of knowledge and information. Do take note that cancer is a continuous struggle between the immune system and the cancer cells. Cancer treatments are meant to assist the immune system in this battle. Any potential treatment—whether conventional or complementary—must be evaluated on a case-by-case basis, with careful consideration of the benefit-risk ratio to ensure both safety and effectiveness.
- The case reports presented reflect the real-life experiences and opinions of other readers or users of the website. The experiences of those readers or users are personal to those particular readers/users and may not necessarily be representative of all readers/users. We do not claim, and you should not assume, that all other readers/users will have the same experiences. Do you own research, consult with relevant medical professionals before attempting to self-treat for any condition.
- Cancer treatment should be part of a multi-modal approach in order to provide the best possible outcome. Diet and lifestyle changes are meant to run alongside conventional treatment. They are complementary, not alternative.
- Cancer care is a team effort with the patient at the centre. Care should be supervised and coordinated by a primary healthcare provider. Patients with cancer should consult with their regular oncologist as well as an integrative provider/oncologist, in addition to their primary care provider and the supporting nurses, dieticians and other allied healthcare professionals.
- While the term 'alternative' might imply opposition to conventional oncology, we prefer 'complementary,' 'integrated,' or 'holistic.' These terms better reflect the role of these strategies as part of a personalized value-added menu of strategies, ensuring the most effective and safe solutions for patients.
- Integrating a repurposed drug doesn't mean rejecting modern medicine — It enhances it and offers a more comprehensive approach to wellness and healing. By combining conventional cancer management with root-cause resolution, this model creates a path to sustained recovery and resilience.
References
- Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263.
- Fizazi K, Tran N, Fein L, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017;377(4):352-360.
- Hussain M, Fizazi K, Saad F, et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2018;378(26):2465-2474.
- Pantziarka P, Vandeborne L, Bouche G. A database of drug repurposing clinical trials in oncology. Front Pharmacol. 2021;12:790952.
- Dogra N, Kumar A, Mukhopadhyay T. Fenbendazole acts as a moderate microtubule destabilizing agent and causes cancer cell death by modulating multiple cellular pathways. Sci Rep. 2018;8(1):11926.
- Hou Z, Huang S, Li Z. Benzimidazoles induce concurrent apoptosis and pyroptosis of human glioblastoma cells via arresting cell cycle. Acta Pharmacol Sin. 2022;43(5):1246-1257.
- Liu J, Liang X, Ren Y, et al. Ivermectin: a systematic review of its antitumor properties and mechanisms. Cancer Cell Int. 2022;22(1):339.
- Draganov D, Gopalakrishna-Pillai S, Chen YR, et al. Modulation of P2X4/P2X7/pannexin-1 sensitivity to extracellular ATP via ivermectin induces a non-classical dendritic cell maturation. J Immunol. 2015;195(5):2316-2329.
- Sweeney CJ, Chen YH, Carducci M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med. 2015;373(8):737-746.
- Abida W, Armenia J, Gopalan A, et al. Prospective genomic profiling of prostate cancer across disease states reveals germline and somatic alterations that may affect clinical decision making. JCO Precis Oncol. 2017;1:1-16.
- Hulscher N, et al. Survey of cancer patients taking ivermectin and mebendazole for 6 months. 2026. [Preprint]
- Martinez P, et al. Targeting the mitochondrial-stem cell connection in cancer treatment: a hybrid orthomolecular protocol. J Orthomolecular Med. 2024;39(3).
- Top 10 Prostate Cancer Fighting Supplements
- Fenbendazole as an Anticancer Agent? A Case Series of Self-Administration in Three Patients -(Case Reports in Oncology 2025)
- Ivermectin, Fenbendazole and Mebendazole in Cancer: 2024 Peer-Reviewed Protocol in Cancer (Journal of OrthoMolecular Medicine 2024)
- Ivermectin and Cancer: 15 Anti-cancer Mechanisms of Action
- Fenbendazole and Cancer: 12 Anti-Cancer Mechanisms of Action
- Ivermectin, Mebendazole, Metformin, High-Dose Vitamin C, Vitamin D, Curcumin, Diet/Lifestyle, and Standard Therapies for Non-BRCA-Mutated Stage 4 Prostate Cancer: A Simulated Double-Blind Randomized Controlled Trial (Grok 2025)
- Fenbendazole vs Mebendazole for Cancer (OneDayMD 2025)
- Fenbendazole vs Ivermectin for Cancer (OneDayMD 2025)
- Turbo Cancer Debunked: What You Need to Know (2025)
- Top 10 cancer fighting supplements
- Joe Tippens Protocol Fenbendazole
- Best Fenbendazole Dosage for Humans: Safety, Side Effects and Efficacy Examined
- Best Ivermectin Dosage for Humans with Cancer or Different Cancer Types
- Fenbendazole and Ivermectin for Cancer: The Ultimate 2025 Guide (OneDayMD 2025)
- The Great Prostate Hoax & Supplements (Urologist 2025)
- Fenbendazole anticancer potential (OneDayMD)
- Treatment Versus No Treatment of Localized Prostate Cancer Had Similar Results Over 15 Years, 1 Question Raised
- Drug Repurposing for Cancer Therapy 2025: From AI-Driven Discovery to Practice-Changing Clinical Trials
- Fenbendazole, Ivermectin and Mebendazole Cancer Success Stories: 700+ Case Reports Compilation of various cancer types (2026 Edition)
- Stage 4 Cancer Remissions with Fenbendazole, Ivermectin and Mebendazole: 300+ Case Reports Compilation of various stage 4 cancer types (2026 Edition)
- Prostate Cancer Research Highlights (2025 - 2026)
- Computational Modeling to Identify Drugs Targeting Metastatic Castration-Resistant Prostate Cancer Characterized by Heightened Glycolysis
- Prostate Cancer in 2026: Risk Modification, Therapeutic Advances, and Emerging Evidence from Repurposed Drug Case Series
- The Great Prostate Hoax - By Richard Ablin and Ronald Piana (Substack 2024)
- Ivermectin, Fenbendazole and Mebendazole for Stage 4 Prostate Cancer: A Case Series of 39 Patients (2026 Update)

Researched and approved by Dr. Peter McCullough.
- Prescribed by licensed medical professionals
- Compounded and dispensed by a licensed US-based pharmacy
- Approved for human use


.png)







Is 34 a good number? I feel like it should be higher, hundreds of people or thousands even. Less than 100 seems so small :(
ReplyDelete