DMSO and the Eyes: A Complete Guide to Every Eye Condition It May Help Organized by Category — From Dry Eyes to Macular Degeneration, Cataracts, Glaucoma, and Retinal Disease
| By OneDayMD | Updated June 2026 | Editorial review and synthesis of clinical, veterinary, and patient-reported data |
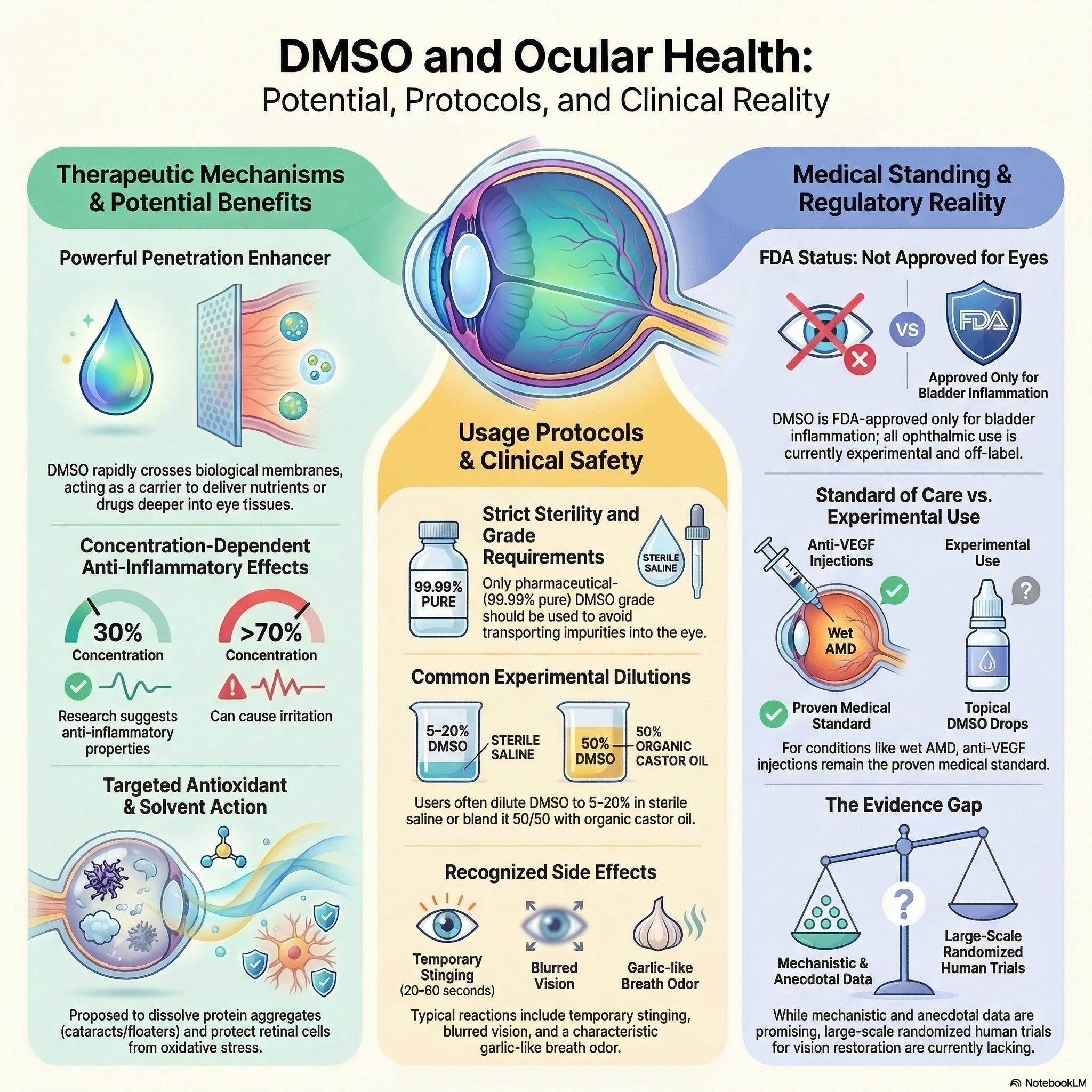
| ⚠️ Medical Disclaimer: DMSO (dimethyl sulfoxide) is FDA-approved only for intravesical treatment of interstitial cystitis. Ophthalmic (eye) use is off-label and experimental. This article synthesizes historical clinical data, veterinary research, animal studies, and patient-reported outcomes — most of which lack modern randomized controlled trials. Self-experimentation on the eyes carries real risk including infection, irritation, and contamination. Always obtain a formal diagnosis and consult an ophthalmologist before pursuing any off-label eye treatment. This article is for educational purposes and does not constitute individual medical advice. |
Introduction
Dimethyl sulfoxide (DMSO) has one of the more unusual histories in modern medicine. Discovered in 1866 and explored intensively in the 1960s, it was on track to become one of the most widely used drugs in America before regulatory restrictions — triggered by a single unrelated death and a high-dose animal eye study — halted most U.S. research into it. Despite this, DMSO never disappeared. It persisted in veterinary medicine, in compounding pharmacies, and in a growing community of patients and integrative practitioners who continued documenting its effects.
Nowhere has that persistence produced a more striking body of reports than in ophthalmology. According to an extensive synthesis by independent researcher and physician A Midwestern Doctor, who compiled and reviewed over 4,700 reader-submitted accounts alongside historical clinical trials, veterinary studies, and mechanistic research, DMSO appears to benefit a remarkably broad range of eye conditions — many of which currently have limited or no effective conventional treatment.
The original analysis is organized narratively, weaving mechanism, history, and patient testimony together across a very long single document. This guide reorganizes that material by clinical category, so that a reader interested in, say, glaucoma or floaters can go directly to the relevant section without reading the entire piece. We have also added current safety context, evidence-tier framing, and updated cross-references to OneDayMD's related DMSO content.
| 📊 How to Read This Article: Each category below opens with the proposed mechanism, followed by the strongest available evidence (clinical, veterinary, or mechanistic), and closes with a representative sample of patient-reported outcomes. Evidence quality varies significantly by category — we flag this throughout rather than presenting all claims as equally well-supported. |
How DMSO Works in the Eye: The Underlying Mechanisms
Before reviewing conditions by category, it helps to understand why a single compound could plausibly affect so many distinct eye disorders. DMSO is not a targeted drug aimed at one receptor or pathway — it is a small, highly polar molecule with a unique combination of physical and biological properties that intersect with the eye in several independent ways:
| Mechanism | Relevance to the Eye |
|---|---|
| Corneal concentration | Radiolabeled studies show DMSO concentrates 2.2–4× higher in the cornea than in blood after systemic administration, explaining why eye improvements are often reported even when DMSO is applied elsewhere on the body. |
| Anti-inflammatory / antioxidant activity | Reduces tissue swelling and protects cells from oxidative stress — relevant to nearly every chronic eye disease. |
| Microcirculation enhancement | The eye has extremely high metabolic demand relative to its blood supply; DMSO improves perfusion to oxygen-starved tissue. |
| Protein stabilization / aggregate dissolution | May help dissolve misfolded protein deposits — relevant to cataracts, floaters, and amyloid corneal disease. |
| VEGF inhibition | Documented inhibition of vascular endothelial growth factor — the same target as costly anti-VEGF injectables used in wet AMD and diabetic retinopathy. |
| Cellular protection from stressors | Protects tissue from heat, cold, radiation, ischemia, and toxic light exposure across multiple animal models. |
| Acetylcholinesterase inhibition | Stimulates parasympathetic tone, increasing tear secretion — relevant to dry eye and Sjögren's-related dryness. |
| Muscle relaxation | May relax overstrained or spasming eye muscles, relevant to twitches, myokymia, and possibly focus disorders. |
| Enhanced drug penetration | A potent carrier molecule that boosts penetration of co-applied steroids, antimicrobials, and antioxidants into ocular tissue. |
| Edema reduction | Draws excess fluid out of tissue, relevant to corneal edema, glaucoma pressure, and post-surgical swelling. |
Category 1: Corneal & Ocular Surface Disorders
Includes: dry eye / Sjögren's-related dryness, corneal abrasions, gelatinous drop-like corneal dystrophy, corneal edema, Fuchs' dystrophy, pterygium, pinguecula, conjunctival cysts
Why This Category Responds to DMSO
DMSO concentrates preferentially in the cornea after systemic or topical administration. Combined with its acetylcholinesterase-inhibiting effect (which increases tear secretion) and its ability to draw out excess fluid (relevant to edema), the cornea and ocular surface represent the eye structures with the most direct mechanistic rationale for DMSO benefit.
Dry Eye Disease
This is one of the most consistently and frequently reported benefits across the patient community. Reader accounts describe DMSO eye drops reducing reliance on commercial artificial tears, resolving chronic dryness within days to weeks, and providing relief in cases — including Sjögren's syndrome — where conventional drops had failed. One reader with Sjögren's reported instantaneous relief upon application after weeks of standard drops providing none. Several reports describe a gradual approach: starting at very low concentrations and slowly increasing strength over months, eventually eliminating the need for artificial tears entirely.
Corneal Abrasions and Severe Surface Pain
One striking account involves a reader with Ehlers-Danlos Syndrome (EDS) and mast cell activation disorder whose brittle corneas left her without enough corneal tissue to hold tears or shield nerve endings. After making a DMSO-hyaluronic acid combination drop, she reported that long-standing floaters dissolved over the course of a month and that a protective film formed over the cornea, reducing constant burning. Another reader with decades of mysterious intermittent eye pain following an old penetrating injury reported the best pain control of their life after three months of DMSO drops, with objective improvement on a Schirmer tear test.
Gelatinous Drop-Like Corneal Dystrophy and Corneal Amyloid
This rare genetic disorder involves amyloid buildup beneath the corneal epithelium and currently has no treatment short of corneal transplant — which can recur. DMSO has an established ability to dissolve amyloid deposits elsewhere in the body, and case reports describe it clearing amyloid that accumulated after corneal transplantation, including in pediatric patients.
Corneal Edema and Fuchs' Dystrophy
Early DMSO trials repeatedly documented resolution of corneal edema. For Fuchs' dystrophy — a progressive, currently incurable condition where the cornea swells with fluid — multiple reader reports describe reduced corneal edema and improved vision with continued DMSO use, although results were mixed and not all users had formal diagnostic confirmation.
Pterygium, Pinguecula, and Conjunctival Cysts
Reports include resolution of a pterygium (a growth of tissue over the cornea) that occurred incidentally after DMSO was applied to the neck for an unrelated issue, a conjunctival cyst, and a German-language report of pinguecula improvement.
| Evidence Strength — Surface Disorders: Moderate for dry eye (large volume of consistent reports plus a clear mechanistic basis); low-to-moderate for edema and dystrophies (small case reports, no controlled trials); anecdotal only for pterygium/pinguecula. |
Category 2: Lens & Structural Disorders
Includes: cataracts, vitreous floaters
Why This Category Responds to DMSO
The lens and vitreous are largely composed of structural proteins (crystallins) and collagen. DMSO's proposed ability to stabilize proteins and dissolve aggregates provides a plausible — though clinically unconfirmed in controlled human trials — mechanism for affecting both cataract-related lens opacity and the protein/collagen debris that forms vitreous floaters.
Cataracts
A 1980 report to the American Academy of Medical Preventics by ophthalmologist Norbert J. Becquet, MD, described treating 200 patients for macular degeneration, macular edema, and traumatic uveitis with notable success using DMSO, helping seed early ophthalmic interest. Reader-submitted reports describe cataracts clearing or stabilizing over a period of months, in some cases allowing scheduled surgery to be postponed or cancelled. One reader specifically combined DMSO with coconut oil and tea tree oil to address Demodex mite involvement they believed was contributing to lens clouding.
Importantly, a separate body of cataract research has investigated lanosterol — a cholesterol precursor — as a standalone agent for dissolving crystallin aggregates. A 2019 controlled study (Daszynski et al., Scientific Reports) found lanosterol alone failed to restore lens clarity in ex vivo human and animal lens models, complicating the simple "lanosterol dissolves cataracts" narrative. DMSO's role may be less about delivering lanosterol and more about its own direct anti-inflammatory and protein-stabilizing action — or a combination of both.
Vitreous Floaters
Floaters are among the most frequently and consistently reported improvements in the community, with multiple accounts of significant reduction or disappearance within days to weeks. One independent Substack author documented a self-experiment using repeated 100% DMSO applications directly to the eyes (a far higher concentration than generally recommended) and reported floaters mostly resolving, alongside only brief stinging and no lasting adverse effects. The previously mentioned EDS patient reported floaters that had been present and visually obstructive for years dissolving over the course of a month using a DMSO-hyaluronic acid drop.
| ⚠️ Evidence Strength — Lens & Structural Disorders: Anecdotal-to-low for both conditions. No controlled human trials confirm cataract reversal or floater elimination via DMSO. The 100% concentration self-experiment described above is well outside typical safety recommendations (most protocols cap at 40–50%) and should not be interpreted as a validated approach. |
Category 3: Retinal & Macular Disease
Includes: macular degeneration, diabetic retinopathy, retinitis pigmentosa, retinal ischemia, retinal artery/vein occlusion, retinal hemorrhage, photoreceptor light damage
Why This Category Responds to DMSO
This is the category with the strongest combination of mechanistic plausibility and modern peer-reviewed animal data. Retinal disease is overwhelmingly driven by three processes DMSO is documented to influence: oxidative stress, abnormal VEGF-driven blood vessel growth, and ischemia (insufficient blood flow). Multiple independent rodent studies — spanning five decades — converge on a consistent protective effect.
Macular Degeneration and Diabetic Retinopathy
The most important recent data point is a 2025 rat diabetic retinopathy study in which subconjunctival injection of 10% and 50% DMSO preserved retinal function and reduced inflammation and cataract risk compared to controls, with the 50% group showing significantly higher electroretinography B-wave amplitude and enhanced flicker responsiveness. DMSO's VEGF-inhibiting properties — also documented in corneal cells after acid burns and abrasions — directly parallel the mechanism of action of anti-VEGF injectable drugs used for wet macular degeneration and diabetic macular edema, two of the costliest chronic ophthalmic treatments in conventional medicine.
Reader reports describe vision improving from roughly 20/200 to 20/50, Amsler grid distortions resolving, and restored night driving ability in macular degeneration cases. As with other categories, these are uncontrolled self-reports.
Retinitis Pigmentosa
This category has the longest-standing formal human trial history. A 1970s trial in approximately 50 patients found roughly 44% had improved visual acuity and 18% had improved visual fields, with some night vision gains persisting for years. However, the most rigorous study available — a 1983 placebo-controlled trial of 123 patients followed for up to 7 years (Garcia et al., Annals of the New York Academy of Sciences) — found no statistically significant benefit across visual acuity, color vision, visual fields, dark adaptation, or electrophysiological testing. This negative controlled result sits in direct tension with the positive open-label data and the more recent anecdotal reports, and should be weighted heavily when evaluating this category.
Retinal Ischemia and Vascular Occlusion
In a rat model, injecting 1.5% DMSO into eyes subjected to 90 minutes of induced retinal ischemia reduced ganglion cell death, suggesting partial protection from ischemia-reperfusion injury. Reader reports include a case of IV DMSO administered after an optic nerve stroke, which the patient credits with preserving vision in the affected eye, and another describing transient vision "grey-outs" following a retinal bleed that resolved within minutes of applying DMSO gel to the eyelid — consistent with a vascular/circulatory mechanism.
Light-Induced Retinal Damage
Multiple independent mouse studies have found DMSO administered before toxic bright-light exposure preserves retinal structure and function — in one study reducing functional loss from 92–93% (untreated) to 30–33% (DMSO-treated). Protection was only observed when DMSO was given shortly before exposure, not after. Reader accounts include resolution of retinal damage from excessive sun exposure and from solar retinopathy following prolonged direct sun-staring.
| Evidence Strength — Retinal & Macular Disease: This is the category with the most rigorous modern animal data (2025 ERG study) and the longest trial history, but also contains the field's one negative placebo-controlled human trial (retinitis pigmentosa, 1983). Mechanistically the strongest category overall; clinically the most contested. |
Category 4: Pressure & Optic Nerve Disorders
Includes: glaucoma, ischemic optic neuropathy, optic neuritis, optic nerve atrophy
Why This Category Responds to DMSO
Glaucoma management centers on lowering intraocular pressure to protect the optic nerve. DMSO's documented fluid-extracting and edema-reducing properties provide a direct mechanism for pressure reduction, while its circulatory and neuroprotective effects parallel its benefits for other ischemic and neurological conditions described in OneDayMD's coverage of DMSO for stroke and brain injury.
Glaucoma
A controlled rabbit study testing 15% DMSO (alone or combined with the steroid fluocinolone acetonide) found it decreased intraocular pressure with no adverse effects to any examined eye structure, while increasing urine output — indicating systemic absorption following ocular application. The 1980 Becquet report to the American Academy of Medical Preventics described favorable results treating macular degeneration and related conditions; separately, a historical case series of glaucoma patients found their intraocular pressure did not rise from DMSO the way it sometimes does with steroids. Reader reports describe pressure normalization without continued medication use and a perceived protective effect on the optic nerve.
Optic Neuritis, Ischemic Optic Neuropathy, and Optic Nerve Atrophy
These conditions appear in the broader review's scope alongside encephalopathic vision loss, reflecting DMSO's documented neuroprotective properties against ischemia and inflammation in central nervous system tissue generally. The optic nerve, as a direct extension of CNS tissue, would be expected to respond similarly to the neuroprotection DMSO demonstrates in stroke and spinal cord injury models — though this category has the least eye-specific human data of any reviewed here.
| Evidence Strength — Pressure & Optic Nerve: Glaucoma has reasonable animal pressure-reduction data and consistent anecdotal pressure normalization reports. Optic nerve conditions (neuritis, atrophy, ischemic neuropathy) rely primarily on extrapolation from DMSO's general neuroprotective profile rather than eye-specific trials. |
Category 5: Inflammatory & Infectious Conditions
Includes: uveitis, iritis, iridocyclitis, episcleritis, choroiditis, conjunctivitis, keratitis (bacterial, fungal, viral), herpes zoster ophthalmicus
Why This Category Responds to DMSO
This category has the strongest veterinary clinical-trial evidence of any group covered in this article, largely because chronic superficial keratitis (CSK) and related inflammatory eye diseases are common and well-studied in dogs and horses. DMSO's combination of anti-inflammatory, antimicrobial, and drug-delivery-enhancing properties make it useful both alone and as a potentiator for conventional anti-inflammatory and antimicrobial drugs.
Chronic Superficial Keratitis (Veterinary Gold Standard)
Multiple controlled veterinary studies found 50% DMSO combined with dexamethasone or prednisolone outperformed either steroid alone for reducing corneal inflammation and neovascularization in dogs with CSK, in some series showing 77.9–90.7% reduction in abnormal blood vessel growth and 95.4% repigmentation of the nictitating membrane. Five-week courses of DMSO combined with tacrolimus produced comparable reductions in inflamed corneal surface area. One clinical trial found 30% DMSO had anti-inflammatory effects on the eye comparable to 0.01% dexamethasone — without steroid-related risks.
Bacterial, Fungal, and Viral Eye Infections
In calves with infectious keratoconjunctivitis, DMSO combined with penicillin matched the effectiveness of dexamethasone-penicillin combinations without steroid risk. In horses, topical DMSO plus itraconazole resolved chronic fungal keratomycosis (keratomycosis) in 80% of treated cases, and a related case report describes full recovery from fungal ulcerative keratitis using DMSO plus fluconazole. For viral disease, DMSO combined with the antiviral idoxuridine (5-IDU) was historically used — and remains available through some compounding pharmacies — to treat herpes simplex keratitis and ophthalmic shingles (herpes zoster ophthalmicus), a serious and difficult-to-treat condition.
Uveitis, Iritis, and Iridocyclitis
A controlled study in dogs with induced uveitis found DMSO reduced both intraocular pressure and fibrin production. Reader reports include a physician (James Miller, MD) who described his own years-long history of synechiae (adhesions) and uveitis flares fully resolving after several months of DMSO use, with no recurrence despite continued reading — an activity that had previously triggered episodes. Another reader with recurring iritis reported resolution using 3% DMSO drops after steroid drops had only provided temporary relief. A Russian study found ultrasound-augmented DMSO delivery effective for iridocyclitis.
Clinical note: Uveitis is typically a downstream sign of another inflammatory or infectious process. The original review emphasizes that thorough workup to identify the underlying cause remains important even when DMSO provides symptomatic relief, both to prevent recurrence and because untreated uveitis can progress to cataracts, glaucoma-causing adhesions, or vitreous changes.
Episcleritis and Chronic Corneal Edema
An early clinical series found 4 cases of severe episcleritis that had failed corticosteroid treatment all responded to topical DMSO, while 4 cases of chronic corneal edema showed partial improvement.
| Evidence Strength — Inflammatory & Infectious: Strongest category overall for controlled evidence, due to multiple veterinary RCTs and head-to-head comparisons against steroids. Human data is primarily case-report level but mechanistically consistent with the animal literature. |
Category 6: Peripheral & Eyelid Conditions
Includes: blepharitis, styes, chalazions, Demodex infestation, skin tags, periorbital psoriasis, eyelid burns, superior oblique myokymia (eye twitches), under-eye bags, periorbital bruising
Why This Category Responds to DMSO
This category draws on DMSO's well-established dermatologic and musculoskeletal properties — anti-inflammatory action, accelerated bruise resolution, muscle relaxation, and antimicrobial effects — applied to the skin and muscle structures immediately surrounding the eye rather than the eye itself.
Blepharitis (Eyelid Inflammation)
A retrospective study of 17 patients using DMSO combined with povidone-iodine (PVP) found all 17 had a partial or complete response within 4–6 weeks with no adverse events; a companion rabbit safety study confirmed the combination caused no adverse effects over a 14-day course. Case reports include a 95-year-old woman with Demodex-related blepharitis unresponsive to other treatments improving within one week of DMSO-PVP, and a 78-year-old man with rosacea-associated blepharoconjunctivitis — who had failed a dozen prior treatments — showing improvement within hours and further gains at one month.
Styes and Chalazions
A pediatric study found DMSO reduced swelling and pain from eyelid styes, and a Russian study confirmed efficacy for inflammatory eyelid disease generally. Multiple reader reports describe styes resolving within 24 hours of a single DMSO application after failing other treatments, and at least one report of chalazion improvement.
Periorbital Psoriasis and Demodex
Reader reports include complete resolution of psoriasis around the eyes and resolution of Demodex-related eyelid issues, sometimes combined with coconut oil and tea tree oil as adjunctive antimicrobial agents.
Superior Oblique Myokymia and Eye Muscle Spasms
This rare, concussion-linked condition causes spontaneous twitching of the superior oblique muscle, distorting vision (including double vision) and posing a driving hazard. A reader with this condition reported DMSO relaxed the spasming muscle and reduced episode frequency over time, a finding corroborated independently by a physician (James Miller, MD) who reported curing chronic eye twitches in his own patients with DMSO. Community reports also describe DMSO enhancing the effectiveness of eye-muscle exercises when applied beforehand.
Burns, Skin Tags, Bruising, and Cosmetic Concerns
DMSO's well-documented burn-healing properties extend to periorbital burns, including one report of a decade-old chemical/heat burn near the eye resolving abruptly with 25% DMSO. Additional reports describe resolution of skin tags and epidermoid cysts on the eyelids, improvement in under-eye bags and wrinkles, periorbital cellulitis resolution, accelerated healing of bruising from orbital fractures in an elderly patient, and even increased eyelash length and thickness.
| Evidence Strength — Peripheral & Eyelid: Moderate for blepharitis (controlled retrospective data) and styes (pediatric study plus consistent reports); anecdotal for cosmetic and muscle-spasm applications, though mechanistically consistent with DMSO's broader dermatologic and musculoskeletal evidence base. |
Category 7: Refractive & Focus Disorders
Includes: presbyopia, nearsightedness, reduced dependence on corrective lenses
Why This Category Responds to DMSO
The proposed mechanism here is muscular rather than structural: DMSO's relaxant effect on the ciliary muscle (which controls lens focusing) may ease the muscle rigidity associated with presbyopia, while reduced corneal/lenticular edema could marginally affect refractive measurements in nearsightedness.
Reported Outcomes
This is the most speculative category in the entire review, with the least direct study support. Reader-reported diopter improvements in the 0.25–1.0+ range have been described for both presbyopia and myopia, generally accumulating gradually over weeks of consistent low-concentration use rather than appearing immediately. The community-reported case of a 71-year-old golfer regaining the ability to read without glasses after using DMSO topically for joint pain (with no direct ocular application) illustrates the proposed systemic-circulation mechanism, though it remains a single anecdotal account.
| ⚠️ Evidence Strength — Refractive Disorders: Weakest category in this review. No controlled studies. Reports are plausible given DMSO's muscle-relaxant properties but should be treated as the least substantiated claims discussed here. |
Safety, Toxicity, and Intraocular Lens (IOL) Considerations
What Controlled Animal and Human Safety Data Show
Despite intense regulatory scrutiny since the 1960s, no study — including high-dose studies in humans and primates — has detected lasting eye toxicity from DMSO at therapeutic concentrations. Key findings include:
| Study Type | Finding |
|---|---|
| Rabbit eyes, 15% DMSO | No adverse effects to any eye structure; decreased intraocular pressure; increased urine output (confirming systemic absorption) |
| Rabbit eyes, 30–100% DMSO | No structural change to iris, cornea, lens, retina, conjunctiva, or lids; 100% caused temporary tearing only |
| 108 human patients, 157 eyes, up to 19 months | No corneal injury, deposits, cataract development, or refractive change; pre-existing glaucoma and cataract patients showed no worsening |
| Intravitreal injection studies (rats) | Concentrations ≤0.2% showed no detectable retinal ERG impairment; 0.5–1.0% caused mild-to-significant but reversible changes |
| Repeated intraocular DMSO injection (rabbits) | Cataracts developed after 6–8 weeks — this is the key data point underlying historical "DMSO causes cataracts" concerns, and it is injection-specific, not relevant to topical drops |
The clinically important distinction is route of administration: injected, repeated, high-concentration DMSO directly into ocular tissue can cause lens changes in animal models. Topical drops, even at high concentrations, have not reproduced this effect in any human study reviewed, likely because topical DMSO dilutes rapidly as it passes through the eye rather than remaining concentrated in one location.
Intraocular Lenses (IOLs) — Post-Cataract Surgery
For patients with artificial lenses from prior cataract surgery, available evidence suggests low-concentration DMSO eye drops are unlikely to pose a problem: dilute DMSO has minimal leaching potential, most common IOL materials show reasonable resistance to DMSO, and the American Academy of Ophthalmology has stated there is no evidence of DMSO harming IOLs. German ophthalmologists using low-dose DMSO drops in IOL patients have reported no issues, and no community reports describe IOL damage — with some instead noting DMSO helped heal complications from eye surgery. High-concentration drops in IOL patients remain an unknown, as lens plasticizer composition and DMSO solubility data are often unavailable from manufacturers. Every source reviewed recommends only low-dose DMSO for IOL patients as a precaution.
| ⚠️ Contact Lens Warning: Contact lenses should never be worn in conjunction with DMSO eye drops. Sufficient time must be allowed between application and lens insertion to ensure no residual DMSO remains on the eye surface to interact with the lens material. |
Drug Interaction Timing
Because DMSO enhances drug penetration, the community standard is to wait at least 2 hours between any prescribed ophthalmic medication and DMSO application, to avoid unpredictable changes in medication potency.
Practical Protocols by Category
Always source pharmaceutical-grade (99.9%+ purity) DMSO stored in glass containers. Begin at the lowest end of any range and increase gradually only if well tolerated.
| Category | Typical Reported Protocol |
|---|---|
| Dry eye / surface | Start at 3–10% in sterile saline; 1 drop, 1–2× daily; increase gradually over weeks |
| Cataracts / floaters | 10–40% in sterile saline; consider adding N-acetylcarnosine or glutathione; 1–2 drops, 1–3× daily |
| Retinal / macular | Low-to-moderate concentration drops (10–20%); some users add systemic/oral DMSO; eyelid application also reported effective |
| Glaucoma | 10–15% drops; physician monitoring of intraocular pressure strongly advised given the stakes of uncontrolled glaucoma |
| Inflammatory / infectious | 30–50% drops, sometimes combined with diluted antimicrobial or anti-inflammatory agents under medical supervision |
| Peripheral / eyelid | 25–70% applied topically with a cotton swab to the eyelid, stye, or affected skin (not into the eye itself) |
| Refractive / focus | Low-concentration drops (10–15%) used consistently over months; least-established category |
For the full standalone protocol guide including the DMSO + castor oil blend and eyelid/topical methods, see OneDayMD's companion article, "DMSO Eye Drops: Complete Guide to Healing Cataracts, Macular Degeneration, Floaters & Glaucoma."
Conclusion
Organizing this material by category makes one thing clear: DMSO's reported eye benefits are not a scattershot collection of unrelated claims but follow a coherent pattern rooted in a small number of underlying mechanisms — corneal concentration, anti-inflammatory and antioxidant action, VEGF inhibition, circulatory enhancement, protein stabilization, and muscle relaxation. Categories where multiple mechanisms converge (inflammatory/infectious conditions, retinal/macular disease) have the strongest supporting evidence, including genuine veterinary RCTs and a 2025 peer-reviewed animal study. Categories relying on a single, more speculative mechanism (refractive disorders, floaters) have the weakest evidence and rest almost entirely on patient report.
None of this substitutes for an ophthalmologist's evaluation, and the one placebo-controlled human trial in this entire body of literature — the 1983 retinitis pigmentosa study — returned a negative result that deserves real weight. But for patients facing conditions where conventional ophthalmology offers little (gelatinous drop-like corneal dystrophy, treatment-resistant blepharitis, certain forms of uveitis), the categorized evidence here may justify a conversation with your eye care provider about a carefully monitored trial.
| Before trying DMSO for any eye condition: (1) Get a formal diagnosis from an ophthalmologist. (2) Source only pharmaceutical-grade DMSO. (3) Start at the lowest concentration for your category. (4) Never replace urgent, sight-threatening care (retinal detachment, acute angle-closure glaucoma, rapidly progressive vision loss) with self-experimentation. (5) If you wear contacts or have an IOL, read the safety section above carefully. |
Sources and Further Reading
Primary Source for This Review
- A Midwestern Doctor — "DMSO Heals the Eyes and Transforms Ophthalmology" (October 2025; updated November 2025)
From OneDayMD
- DMSO Eye Drops: Complete Guide to Healing Cataracts, Macular Degeneration, Floaters & Glaucoma
- DMSO: A Versatile Compound for Eye Health and Vision Restoration
- DMSO for Stroke, Brain Injury, Spinal Cord Trauma, and Ischemic Damage
- DMSO 101: Benefits, Uses, Dosage and Side Effects
From A Midwestern Doctor (The Forgotten Side of Medicine)
- The Remarkable History and Safety of DMSO
- DMSO is a Miraculous Therapy for Chronic Pain and Musculoskeletal Injuries
- How DMSO Treats "Incurable" Autoimmune and Contractile Disorders
- DMSO Could Save Millions From Brain Injury and Neurological Disease
Key Peer-Reviewed and Reference Sources
- Hoang et al. Application of Dimethyl Sulfoxide as a Therapeutic Agent and Drug Vehicle for Eye Diseases. J Ocul Pharmacol Ther. 2021. PMID 34314611
- Hwang et al. Therapeutic Potential of Dimethyl Sulfoxide via Subconjunctival Injection in a Diabetic Retinopathy Rat Model. In Vivo. 2025. PMC11705140
- Garcia et al. Placebo-controlled trial of DMSO in retinitis pigmentosa (123 patients, up to 7 years). Ann N Y Acad Sci. 1983.
- Daszynski et al. Failure of Oxysterols Such as Lanosterol to Restore Lens Clarity from Cataracts. Sci Rep. 2019. doi:10.1038/s41598-019-44676-4
| Important Disclaimer: This article discusses dimethyl sulfoxide (DMSO), an FDA-approved solvent for certain medical uses (e.g., interstitial cystitis), but not approved for ophthalmic (eye) application. Evidence for eye benefits combines historical small clinical trials, veterinary research, animal studies, and a large volume of patient-reported outcomes that have not undergone modern controlled trials. The one placebo-controlled human trial available (retinitis pigmentosa, 1983) found no significant benefit. Self-experimentation carries risks including irritation, infection, and contamination. Always consult an ophthalmologist before pursuing any off-label eye treatment. DMSO is not a substitute for proven therapies such as anti-VEGF injections, cataract surgery, or glaucoma medications. |
Article published June 2026 by OneDayMD. Editorial synthesis and categorization of third-party research and reporting.


.png)







Comments
Post a Comment