Ivermectin and Mebendazole for Skin Cancer: Case Series of 16 Case Reports (May 2026 Update)
In an era where conventional cancer treatments often come with significant side effects and variable success rates, alternative therapies are gaining attention for their potential accessibility and lower toxicity. This exploration delves into the emerging use of topical ivermectin—a well-established antiparasitic medication—for treating skin cancers such as basal cell carcinoma, squamous cell carcinoma, and melanoma. Drawing from a compilation of anecdotal success stories, case reports, and preliminary scientific insights, we examine how this affordable, over-the-counter option might disrupt traditional dermatological approaches. While not a substitute for professional medical advice, these narratives highlight patient-driven innovations that challenge the status quo, prompting a closer look at ivermectin's multifaceted mechanisms and real-world applications.
Case Presentations
IVERMECTIN and MEBENDAZOLE and Topical Ivermectin Testimonial - 66 year old Texas nurse with Basal Cell Carcinoma at the nose/cheek junction reports after 4 months - cancer free!
Case 15 - 2026: 94-year-old grandmother with recurrent skin cancer on her scalp
@pro_groups shared on X.com in April 2026:
IVERMECTIN and FENBENDAZOLE Testimonial - 81 year old woman living in Shanghai, CHINA with Stage 4 Melanoma, reports after 3 months! Most cancer is gone.
IVERMECTIN and MEBENDAZOLE Testimonial - 69 year old man from Peru with Stage 4 Melanoma (Anorectal) reports after 4 months - dramatic improvement in quality of life!
IVERMECTIN and MEBENDAZOLE Testimonial - 59 year old Michigan woman with Skin Cancer (SCC and BCC) sees major improvements after 4 months
Initiated Fenbendazole: 222 mg daily. PC begins self-directed therapy.
May 2024: PET-CT: Resolution of clavicular and mediastinal metastases. Persistent para-aortic disease (SUV max 7.04). Unremarkable brain CT.
Fenbendazole 222 mg daily. Significant partial response to fenbendazole monotherapy.
June 8, 2024: Genetic testing confirmed NRAS mutation, CDKN2A gene )p.M53l variant).
June 10, 2024: Blood Panel: Transient elevation of liver enzymes (ALT/AST).
Fenbendazole 222 mg daily. Liver enzyme elevation likely due to tumor lysis; therapy continued.
June 20, 2024: Dose Adjustment: Fenbendazole increased to 444 mg daily (222 mg twice per day). Fenbendazole Dose Escalation. Dose increased to drive further therapeutic response.
Sept 17, 2024: PET-CT: Resolution of cutaneous leg lesion. Further reduction in para-aortic node (SUV max 5.89). No new disease.
Fenbendazole 444 mg daily. Continued favorable response.
Blood Panel: Liver enzymes returned to normal range.
Fenbendazole 444 mg daily. Normalization confirms the transient nature of the enzyme elevation, ruling out hepatotoxicity.
Sept 20, 2024: Immunotherapy Initiated: Began combination therapy with Nivolumab/Relatlimab (monthly infusions).
Immunotherapy Introduced. Standard-of-care immunotherapy added to consolidate gains.
Jan 10, 2025: CT & PET Scans: No nodal or metastatic disease detected. Para-aortic node no longer avid (SUV max 2.3). Clear brain scan.
Immunotherapy complete. Complete Metabolic Response Achieved.
May 15, 2025: Follow-up: PC is active, in excellent health, and remains cancer-free. Immunotherapy-induced colitis fully resolved. No active cancer treatment.
Durable Complete Response.
Case Presentation and Clinical Course
Conclusions: The Foundational Role of Fenbendazole
- Source: https://t.co/WGllfQFysg
- Description: Posted on March 29, 2025, by@MakisMD, this highlights an Australian man with Stage 4 malignant melanoma with metastases to multiple sites. He reportedly achieved a "cancer-free" status after 12 months using ivermectin and fenbendazole.
"As I’ve told you, my wife had stage 4 melanoma with mets to lymph nodes. She started taking ivermectin before you released your protocols, 1mg/kg. Weeks later you published your protocols and I bumped her to 2mg/kg. I added 444 mg of fenbendazole. Her last pet scan was approximately 6 months where she was cancer free. Her oncologist was all smiles, but I never told him I was giving her the protocol. She continues to take .5mg/kg of ivermectin 6x week and 3x week of 444 mg fenbendazole. She was taking immunotherapy for about a year before I read about ivermectin. Her lesions were having moderate response to the immunotherapy per pet scans. After putting her on ivermectin, 45 days later with a pet scan she presented cancer free. We were blown away. I almost cried. Doctor this is the hope you’ve given us. Your stories continue to give my wife confidence. It is like a big dark cloud we lived with was lifted."
IVERMECTIN, FENBENDAZOLE and MEBENDAZOLE Testimonial:



In this December 2024 case report published by Canadian Oncologist Dr. William Makis on X.com, we note the pictorial resolution of basal cell cancer [BCC] to the point that the patient may have to cancel his appointment for a planned surgical removal. One cannot surgically remove a basal cell cancer [BCC] that no longer exists.
This gentleman reports he is a long-time reader of Dr. Makis and was particularly interested in his reports of Fenbendazole and Ivermectin. He contracted basal cell cancer on his face in February or March of 2024, and did what most of us would do - he booked an appointment with his GP in June 2024, apparently the first available.
The soonest he could get scheduled for the Dermatology referral was sometime in November. Having nothing to lose, he decided to apply Fenbendazole paste per the articles he had previously read, and to his pleasant surprise the persistent non-healing skin cancer of seven months began to shrink in size.
 |
| FenBen Treatment from September 25 through October 28, 2024 |
By the time of his November Dermatology appointment, there was very little to biopsy, yet it was done. He reports the Dermatologist was not the least bit interested in his tumor shrinkage with the Fenbendazole paste. Instead, the Dermatologist booked him for a tumor removal appointment three months later in February 2025.
The patient continued to apply the paste for the next month following the November biopsy, and here is what the BCC looked like as of December 6, 2024.
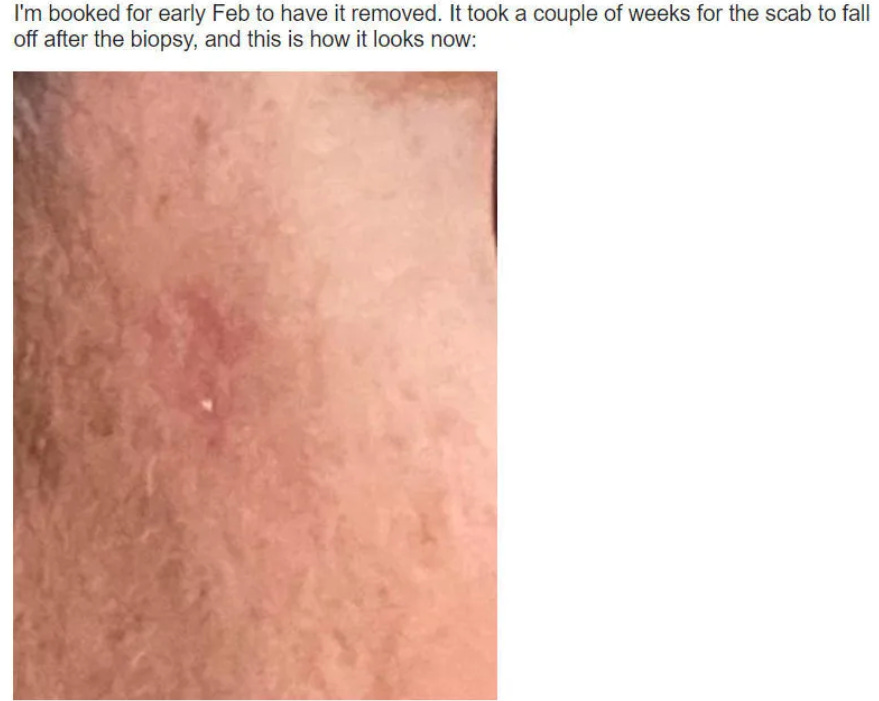
Result of FenBen Topical Treatment from September 25 through December 6, 2024
He writes,
“I’m still treating it once a day with Safeguard 10% Fenbendazole and it seems to still be improving. So I’m undecided about whether I need to have anything removed. I guess I’ll see how it goes over the next while. Maybe it’s deep into the tissue despite having improved the surface cells. No idea.”
Dr. Makis writes in response that patients who take matters into their own hands seem to do better.


 |
| source: https://substack.com/home/post/p-155091883 |

In September 2021, I went to the cancer clinic to get my second PET scan done after receiving the news in March 2021 that I have been diagnosed with cancer, and learnt that day that my tumor has shrunk to half the size it first was. There were still signs of lymph nodes increasing or being classified as unknown results. I continued the use of the fenben protocol along with a whole bunch of other supplements to take on a daily basis, as within 5 months results improved in comparison to a whole year of fighting off the protocol before with little to non improvement in results. I strongly believe in this protocol and in case you wondered – I am not on any chemotherapy/radiation/immunotherapy or any other western medicine use – this is a full on natural and holistic journey I went on, and I am happy to share my current protocol with all cancer patients out there:
- Serrapeptase (at midnight)
- Vit D & K2, Tudca 500mg, Graviola 1ml (on an empty stomach)
- Varies supplementation with breakfast (like Vit C & B complex, probiotics, fish oil, curcumin, etc. along with fenben 888mg)
- Multi-vitamin, turkey tail extract, fenben 888mg, and B17 apricot seed (with dinner)
- Some more other supplements just before bed (like magnesium, Vit C, Graviola, high dose of melatonin, coffee enemas, etc)
- Detox baths (1 x week)
- Frequency music (before bed designed to kill cancer cells)
- Mainly following a plant-based diet
- Protein intake is limited to certain meats
- Fresh whole foods/vegetables
- Healthy fats only
Case 2: October, 2022
In February and March of this year I was diagnosed with stage four melanoma. It had metastasized to my brain, lymph nodes, right lung, adrenal gland and right hip. My daughter pointed me to Joe’s story and this site. I started taking the fenbendazole protocol even before my oncologist gave me her treatment plan using Immuno therapy. The oncologist said that it had about a 30% success rate but not to expect any great results on the first scan after 4 treatments.
I had a PET scan last week and the results were almost too good to be true. Cancer basically gone. The tumor in my right lung had shrunk to less than half the size it was on the first PET scan. The uptake on that tumor decreased from 19.9 to 2.6. I was told by her that an uptake of less than 4.0 is no longer considered as cancerous.
I have been on the fenbendazole protocol for 166 days now. I received 4 immunotherapy injections using 2 different drugs. I can’t say for sure what definitively gave me these great results. Draw your own conclusions but I think the fenbendazole was largely responsible for the great results.
Case 1: January, 2022
At first me and my partner were unsure about trying alternative treatments in addition to the radiation my partner receives. With the help from a holistic healer and referrals from a couple of people in our community, we found out about the fenbendazole protocol and started to add the protocol along with a few other supplements to my partner’s daily intake/routine to aid in fighting the skin cancer on his neck.
Topical Ivermectin and Skin Cancer
- Breast Cancer
- Head and Neck Cancer
- Skin Cancer
 Ivermectin Paste For Melanoma
frontiersin.org/journals/oncol
Ivermectin Clears Skin Cancers
pmc.ncbi.nlm.nih.gov/articles/PMC75
Ivermectin Use In Dermatology
pmc.ncbi.nlm.nih.gov/articles/PMC83
Speaker: Dr William Makis, MD
Ivermectin Paste For Melanoma
frontiersin.org/journals/oncol
Ivermectin Clears Skin Cancers
pmc.ncbi.nlm.nih.gov/articles/PMC75
Ivermectin Use In Dermatology
pmc.ncbi.nlm.nih.gov/articles/PMC83
Speaker: Dr William Makis, MD"Topical Ivermectin Will Completely Heal Skin Cancer...The Lesion Will Change, Get Smaller & Fall Off Completely."
— Valerie Anne Smith (@ValerieAnne1970) October 30, 2025
"You Can Literally Use It For Any Inflammatory Or Autoimmune Skin Condition."
"It Comes As A 1% Prescribed Cream Or Buy The Over The Counter 1.87% 'Horse Paste.'… pic.twitter.com/wjTlz7eqFC
Conclusion
The anecdotal evidence surrounding ivermectin for skin cancer paints an intriguing picture of a simple, low-cost intervention that may hold untapped potential in dermatology and oncology. From rapid lesion resolutions to remissions in advanced cases, these stories underscore the need for innovative thinking beyond traditional paradigms. Yet, as with any emerging therapy, caution is paramount—consulting healthcare professionals and prioritizing evidence-based research remains essential to separate hope from hype. Ultimately, if validated through rigorous studies, ivermectin could redefine accessible cancer care, empowering individuals to take proactive roles in their health journeys.
✔ Treats Acne, Rosacea, and Dermatitis
✔ Reduces Inflammation
✔ Extra-Strength Formula
✔ Doctor-Prescribed
A dermatologist-formulated topical treatment combining three FDA-approved ingredients: Azelaic Acid, Ivermectin, and Metronidazole to target redness, inflammation, and irritation caused by rosacea, lice, acne, and other inflammatory skin conditions.

.png)








Comments
Post a Comment