Base Spike Detox Protocol: Nattokinase, Bromelain, and Curcumin for Clearance of Persistent SARS-CoV-2 Spike Protein (2026)
A clinical review of the evidence base, dosing rationale, safety considerations, and monitoring strategy for the Base Spike Detox regimen in long COVID and post-vaccine injury syndromes — updated June 2026.
Persistent SARS-CoV-2 spike protein — derived from infection, vaccination, or both — has been proposed as a pathophysiological driver of long COVID and post-vaccine inflammatory syndromes. Dr. Peter McCullough, a board-certified internist and cardiologist, has developed a three-agent over-the-counter regimen termed the "Base Spike Detox" that combines nattokinase (2,000 FU twice daily), bromelain (500 mg once daily), and nano/liposomal curcumin (500 mg twice daily) to promote enzymatic degradation and reticuloendothelial clearance of spike protein and its fragments. This article reviews the mechanistic rationale, available in vitro and clinical evidence, dosing guidance, drug interaction profile, monitoring strategy, and frequently asked questions. In the absence of completed large randomized controlled trials, these recommendations represent an evidence-informed clinical approach to a population for whom no approved targeted therapy currently exists. All patients should consult a qualified physician before initiating this or any therapeutic protocol.
Base Spike Detox Protocol
The Base Spike Detox was introduced by Dr. Peter McCullough for patients who have experienced COVID-19 infection one or more times, received one or more COVID-19 vaccines, or both, and who suspect that persistent SARS-CoV-2 spike protein may be contributing to ongoing symptoms. Based on emerging scientific literature1 and clinical observation, Dr. McCullough identified three over-the-counter compounds as essential in combination:
| Agent | Dose | Frequency | Timing |
|---|---|---|---|
| Nattokinase | 2,000 FU (≈100 mg) | Twice daily | Empty stomach |
| Bromelain | 500 mg | Once daily | Empty stomach |
| Nano/Liposomal Curcumin | 500 mg | Twice daily | With food |
Duration: Minimum 3 months; many patients require 6–12 months or longer. Continue if well-tolerated; symptoms may recur with reinfection. Progress can be tracked via the SARS-CoV-2 Spike Protein Antibody (Semi-Quantitative) test available through Labcorp.
The therapeutic objective of the protocol is to initiate treatment while the body's natural reticuloendothelial system clears spike protein and its fragments. Dr. McCullough has stated that patients can get a head start by self-initiating the Base Spike Detox while organizing appointments with a physician. Additional prescription agents — including ivermectin, hydroxychloroquine, N-acetylcysteine (NAC), low-dose naltrexone, and anticoagulants — may be added based on clinical evaluation and syndrome characterization.
- Anticoagulants / blood thinners (warfarin, apixaban/Eliquis, rivaroxaban/Xarelto, dabigatran): Use only under physician supervision. Nattokinase is an oral fibrinolytic; bromelain prolongs prothrombin time. Monitor for bruising and mucosal bleeding.
- Aspirin: Has antiplatelet activity. Consult your physician before combining with nattokinase or bromelain.
- Soy allergy: Nattokinase is derived from fermented soybeans — avoid if allergic to soy.
- Pregnancy, breastfeeding, and children: Do not take without direct physician guidance.
- Women of childbearing potential without contraception: Avoid unless directed by a physician.
- Low blood pressure: Nattokinase may modestly lower blood pressure. Monitor if you are hypotensive or on antihypertensive medications.
- GI intolerance: Reduce dose if gastrointestinal symptoms develop. Bromelain on an empty stomach may cause nausea in sensitive individuals.
- Bleeding disorders (e.g., hemophilia): Contraindicated without specialist supervision.
Additional Agents (Prescription & Adjunctive)
Based on clinical evaluation, the following may be added to the base regimen:
- Ivermectin (0.2–0.3 mg/kg daily, prescription): For cardiopulmonary symptoms and spike-induced hemagglutination reversal.
- N-Acetylcysteine (NAC): For additional antioxidant and mucolytic support.
- Low-Dose Naltrexone (LDN): For immune modulation in post-viral syndromes.
- Hydroxychloroquine (HCQ): In select patients with autoimmune-like features, per physician assessment.
- Anticoagulants / antiplatelets: For documented micro-clotting or thrombotic complications, under physician supervision.
Patients who have been on the base protocol for six months or more without adequate improvement are encouraged to review the FLCCC I-RECOVER Protocol for additional management strategies, and to seek a physician experienced with post-COVID syndromes via the Find a Doctor directory.
Nattokinase and SARS-CoV-2 Spike Protein: Mechanistic Evidence
Nattokinase is a serine protease derived from Bacillus subtilis natto, traditionally produced during the fermentation of soybeans. Its fibrinolytic properties have been documented in multiple human studies, and it has attracted attention in the post-COVID context for its capacity to degrade spike protein directly.
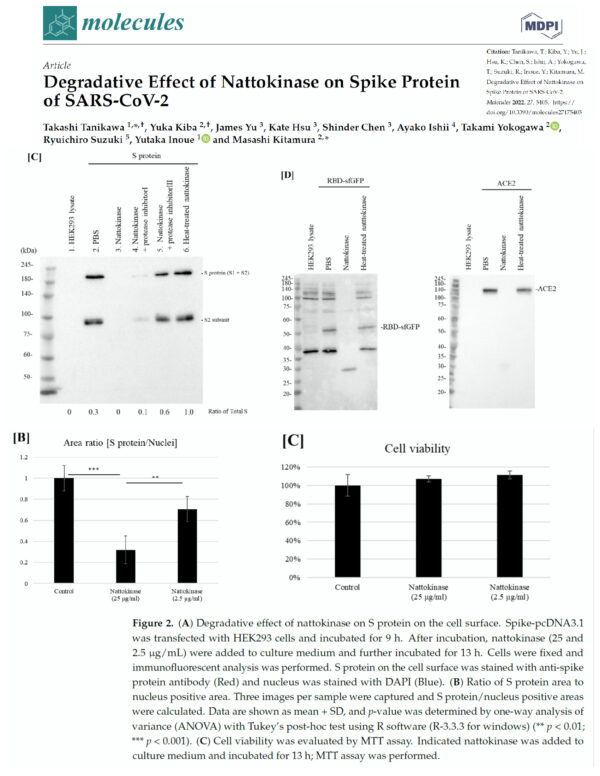
Tanikawa et al. (2022) — In Vitro Degradation Studies
Tanikawa and colleagues4 examined the effect of nattokinase on the spike protein of SARS-CoV-2 in two complementary experiments. In the first, they demonstrated that spike protein was degraded in a time- and dose-dependent manner in a cell lysate preparation analogous to conditions in a vaccine recipient. In the second, nattokinase degraded spike protein present in SARS-CoV-2-infected cells. These findings were reproduced in a related study by Oba and colleagues (2021).
Pharmacokinetic Considerations
Nattokinase is dosed in fibrinolytic units (FU) per gram and potency varies according to product purity. Kurosawa and colleagues demonstrated in human subjects that a single oral dose of 2,000 FU significantly elevated D-dimer concentrations at six and eight hours post-administration, and increased blood fibrin/fibrinogen degradation products at four hours (p < 0.05 for each). This provides a pharmacodynamic rationale for the empiric twice-daily dosing of 2,000 FU.
Full pharmacokinetic and pharmacodynamic characterization is incomplete. However, several years of market experience as an over-the-counter supplement suggest an acceptable safety profile with the primary caveat of enhanced bleeding risk, particularly with concurrent antiplatelet or anticoagulant therapy.
A widely circulated fact-check claimed there is no evidence nattokinase dissolves spike protein in the human body — while simultaneously citing the Tanikawa et al. (2022) in vitro study described above, which demonstrated exactly that in a cell-based model. In vitro studies are frequently the first step before human trials; they are not disqualifying outliers. We agree that large randomized controlled trials are the required next step, and that nattokinase is not a curative agent. Over 250 nattokinase studies exist on PubMed. We encourage readers to review the primary literature and consult their physician.
Ivermectin, Spike Protein, and Hemagglutination Reversal
Former NIH researcher David Scheim, PhD, proposed early in the pandemic that SARS-CoV-2 spike protein was acting as a molecular grappling hook, aggregating circulating red blood cells (RBCs) into chains and clumps — a process termed hemagglutination (HA). This mechanism was proposed to explain impaired oxygen transport and the finding of micro-clots in pulmonary vasculature.
Boschi et al.6 provided additional mechanistic support for spike-mediated hemagglutination. Critically, the same research demonstrated that ivermectin could reverse this effect:
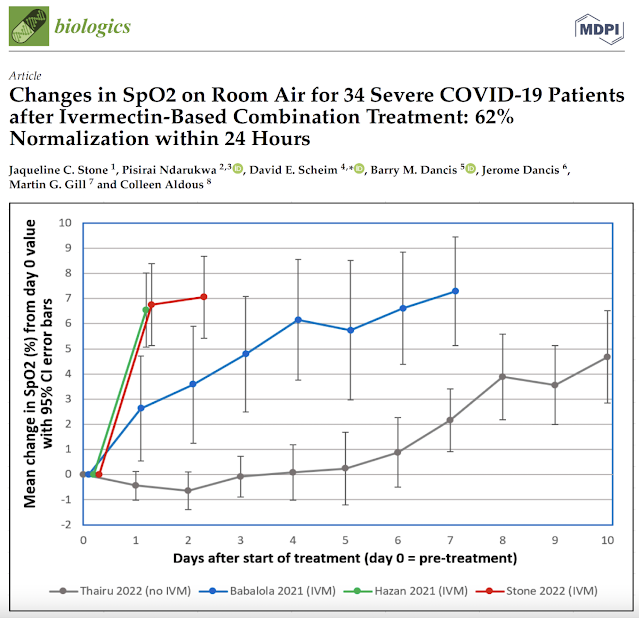
Stone et al.7 described prompt improvement in oxygenation in patients administered ivermectin, with published SpO2 curves showing a 62% normalization rate within 24 hours in severe COVID-19 patients. The rapidity of this physiological effect — too fast to be explained by antiviral activity — suggests a direct anti-spike protein mechanism, consistent with hemagglutination reversal.
For patients with persistent cardiopulmonary symptoms on the base protocol, Dr. McCullough recommends considering ivermectin at 0.2–0.3 mg/kg daily (prescription required). This is consistent with guidance from the FLCCC I-RECOVER protocol for long COVID management.
Monitoring Protocol Progress
SARS-CoV-2 Spike Protein Antibody (Semi-Quantitative) Test — Available through Labcorp in most US states. Order online and visit a local draw site. Healthlabs.com also offers this test.
- Establish a baseline reading before starting the protocol.
- Retest at 3 months and again at 6 months.
- A declining antibody level is the primary measurable marker of protocol efficacy.
- Symptom improvement is the primary clinical marker; antibody titers are confirmatory.
- If antibody levels remain elevated and symptoms persist, consider adding ivermectin or NAC per physician guidance.
Note: The standard COVID-19 IgG test ordered for vaccination status ("Spike IgG") and the Semi-Quantitative Spike Protein Antibody test are not identical. Request the semi-quantitative version to track changes over time with a numeric value.
Dr. Robert W. Enzenauer, MD, MPH, reported in September 2024 that after six months on the McCullough protocol his spike antibody level fell from 1:25,000 (March 2024) to 1:740 — a reduction of approximately 97%. This type of serial quantitative monitoring provides objective data to guide treatment duration decisions.
Reported Case Observations
The following accounts are from physicians and patients who have reported outcomes with the Base Spike Detox protocol. These are observational reports, not controlled clinical data. They are presented to illustrate the range of clinical experiences reported; individual results may vary significantly.
Physician Report: Dr. Robert W. Enzenauer, MD, MPH
"I am a physician who received the Pfizer vaccine in 2020, 2021, and again in 2021 to continue working at a hospital in Colorado. I am happy to report: in March 2024, my spike antibody was 1:25,000. After six months on the McCullough protocol, my spike antibody fell to 1:740 in September 2024." — Dr. Robert W. Enzenauer, MD, MPH · September 2024 · via thefocalpoints.com
Case Study: Dr. Bruce Boros, MD (Internist & Cardiologist, Florida Keys)
Dr. Bruce Boros, an internist and cardiologist who brought modern cardiology to the Florida Keys, treated acute COVID-19 patients with high-dose ivermectin during the pandemic and observed rapid clinical resolution, including imaging evidence of pulmonary improvement in high-risk patients.
Later, Dr. Boros — age 75 and unvaccinated — developed symptoms consistent with long-COVID syndrome: cognitive fog, fatigue, and diminished energy that caused concern about cognitive decline threatening his medical practice. Following a discussion with Dr. McCullough regarding the science of the Base Spike Detox, Dr. Boros initiated the Ultimate Spike Detox from The Wellness Company. Building on a pre-existing supplement regimen and prior ivermectin treatment, he reported resolution of his long-COVID symptoms within weeks, with similar outcomes observed in his own long-COVID patients.
Source: petermcculloughmd.substack.com
Additional Patient Reports
"A friend in Ards had the same problem. Bedridden. Put him on Dr. McCullough's Spike Protein Removal protocol and in 3 months he was back working in construction." — Ni Skies · X/Twitter · October 2025
"I took one shot and my leg swelled up to 3× its normal size. It didn't resolve until I found McCullough's bromelain-based spike detox regimen — the swelling resolved within a week." — Anonymous patient report · X/Twitter · February 2025
"I had a blood clot in my eye. Nothing seemed to dissolve it until I started the Spike Detox product by The Wellness Company. About a week after starting, I noticed slight improvement in vision. The clot was completely dissolved in approximately three weeks." — Keith (Registered Nurse) · Substack comment · November 2024
"I never took the vaccine and don't have COVID symptoms. I simply woke up one morning and couldn't see out of my left eye. I contacted Dr. Kory's clinic and was placed on this protocol, which also included ivermectin (0.4 mg/kg). My leg swelling resolved after approximately six weeks." — Anonymous · Blogger comment · September 2025
The above reports represent individual observational accounts. They have not been independently verified and are subject to recall bias, placebo effect, and natural disease resolution. They should not be interpreted as clinical evidence of efficacy. Large, randomized placebo-controlled trials are required to establish efficacy conclusively and are, as Dr. McCullough notes, likely five or more years away. These accounts are presented to reflect the range of patient experiences reported with this protocol.
COVID-19 Vaccine Myocarditis Research: Award Recognition
A preprint co-authored by Dr. McCullough, titled Autopsy Proven Fatal COVID-19 Vaccine-Induced Myocarditis,3 was recognized with first place in the Medicine and Pharmacology (Cardiac and Cardiovascular Systems) category by Preprints.org at their 2023 Most Popular Preprints Award.2
Preprints.org serves as an early-dissemination platform for scholarly research prior to formal peer review, facilitating scientific communication and enabling rapid community feedback. The awarded study examined fatal myocarditis cases confirmed via autopsy following COVID-19 vaccination, contributing to the evidence base on rare but serious cardiac adverse events associated with mRNA vaccination, particularly in younger males.
The peer-reviewed version was subsequently published in the European Journal of Heart Failure.3
Frequently Asked Questions
-
1. What is the McCullough Protocol Base Spike Detoxification? +
A regimen developed by Dr. Peter McCullough to support the body in degrading and clearing persistent SARS-CoV-2 spike protein arising from infection, vaccination, or both. The core "Base Spike Detox" uses three natural compounds: nattokinase (direct spike protein degradation via fibrinolytic/proteolytic activity), bromelain (fragment clearance and anti-inflammatory effects), and nano/liposomal curcumin (inflammation reduction and immune modulation). The regimen is designed as a foundation to which prescription agents may be added based on clinical evaluation.
-
2. When do I take each supplement — with food or on an empty stomach? +
Nattokinase and Bromelain are proteolytic enzymes that should be taken on an empty stomach for optimal absorption and to avoid competition with dietary proteins. Nano/Liposomal Curcumin is fat-soluble and should be taken with food containing some fat to maximize bioavailability. Standard curcumin has very poor oral bioavailability; the nano or liposomal formulations specified in this protocol are substantially better absorbed.
-
3. How long should someone follow the protocol? +
Dr. McCullough recommends a minimum of 3 months, with many patients requiring 6–12 months or longer, depending on symptom persistence, the number of prior infections or vaccine doses, and spike protein antibody levels. The protocol can be continued indefinitely if well-tolerated. Progress should be tracked with the SARS-CoV-2 Spike Protein Antibody (Semi-Quantitative) test at baseline and at 3–6 month intervals.
-
4. Can you take Ultimate Spike Detox on blood thinners (Eliquis, Xarelto, warfarin)? +
According to Dr. McCullough (X/Twitter, 2025): the combination is used in clinical practice with anticoagulants — including apixaban, rivaroxaban, dabigatran, and warfarin — in patients with thrombotic complications from SARS-CoV-2 and long COVID, but only under physician supervision. The primary safety concern is bleeding. When signs of excessive mucosal bleeding or cutaneous bruising appear, the dose of the spike detox supplement or the anticoagulant should be reduced according to the physician's judgment. Never self-adjust anticoagulant dosing without medical guidance.
-
5. Can I take this protocol if I'm on blood pressure medications? +
These medications are not direct anticoagulants, so the bleeding risk concern is lower than with warfarin or apixaban. However, nattokinase may modestly lower blood pressure through fibrinolytic pathways, which could augment the effect of antihypertensive drugs. Inform your physician before starting, and monitor blood pressure regularly when initiating the protocol. Individual consultation is required.
-
6. I never had the vaccine. Should I still do this protocol? +
Yes — the protocol was designed for individuals who have had COVID-19 infections, vaccines, or both. Persistent spike protein from natural infection (not only vaccination) may contribute to long-COVID symptoms. Dr. McCullough has stated that the protocol applies to anyone with suspected lingering spike protein regardless of vaccination status. If you are asymptomatic and have not had a documented COVID infection, the rationale for prophylactic use is weak; discuss with a physician.
-
7. I'm reacting badly when starting the protocol — should I stop? +
Some practitioners describe a temporary worsening of symptoms early in the protocol, sometimes referred to as a Herxheimer-like reaction. If symptoms are mild and tolerable, a common approach is to reduce the dose by half and gradually increase over 2–4 weeks. If you experience significant bleeding, severe GI distress, allergic reaction, or any alarming symptom, stop immediately and consult a physician. Do not continue if you are unsure — seek professional guidance.
-
8. Can serrapeptase replace nattokinase for those who cannot tolerate it? +
Serrapeptase is a proteolytic enzyme used in some similar contexts, and some practitioners substitute it when nattokinase is contraindicated or not tolerated (e.g., soy allergy, significant hypotension). However, serrapeptase is not part of the McCullough Base Spike Detox protocol, and evidence for its direct spike protein degradation activity is less developed than for nattokinase. Discuss substitution options with a knowledgeable physician.
-
9. What is the ivermectin dosage for long-COVID / spike detox? +
When ivermectin is added to the base protocol, Dr. McCullough and the FLCCC I-RECOVER protocol recommend 0.2–0.3 mg/kg once daily (prescription required). Duration varies by clinical response, typically ranging from weeks to several months. Ivermectin should be taken with food. A physician should prescribe and monitor this therapy, particularly in patients on concurrent medications or with underlying cardiovascular conditions.
-
10. Is there a test to monitor whether the detox is working? +
Yes. The SARS-CoV-2 Spike Protein Antibody (Semi-Quantitative) test is available through Labcorp in most US states — order online and visit a local draw site. Establish a numeric baseline before starting, then retest at 3 and 6 months. A declining titer over time is the primary measurable marker. Note: this is distinct from the standard COVID-19 IgG test used for vaccination status; specifically request the semi-quantitative version.
-
11. I've been on the protocol for many months with persistent symptoms — what next? +
Consider the following escalation steps with physician guidance: (1) Add ivermectin (0.2–0.3 mg/kg daily); (2) Add NAC (600–900 mg twice daily) for additional antioxidant support; (3) Consider low-dose naltrexone (LDN, 1.5–4.5 mg at bedtime) for immune modulation; (4) Review the FLCCC I-RECOVER Protocol for a broader management framework. Seek a physician experienced with post-COVID syndromes via the FLCCC provider directory or The Wellness Company telehealth platform.
-
12. Are children or adolescents able to use this protocol? +
The Base Spike Detox protocol is not recommended for children under 18 without direct physician supervision. Pediatric dosing has not been formally established for this combination. If you are concerned about spike protein exposure in a child, consult a physician familiar with this area — the FLCCC provider directory or The Wellness Company telehealth platform may help identify appropriate specialists.
-
13. Should asymptomatic, unvaccinated people use this protocol preventively? +
The protocol is designed for individuals who suspect persistent spike protein is causing problems — from infection, vaccination, or exposure. There is no established evidence base supporting prophylactic use in truly asymptomatic, unvaccinated individuals with no COVID history. The supplements are generally well-tolerated, but routine preventive use in this group is a personal decision best discussed with a physician.
Conclusion and Key Takeaways
In the absence of completed large randomized placebo-controlled trials — which remain years away — no definitive therapeutic claims can be established for the Base Spike Detox protocol. What exists is a mechanistically coherent rationale supported by in vitro evidence (nattokinase degradation of spike protein; ivermectin reversal of hemagglutination), an established human pharmacodynamic profile for nattokinase, a published clinical review in Cureus,1 and a growing body of observational case reports.
For clinicians and patients navigating post-COVID and post-vaccine syndromes now — without the option of waiting for long-term trial data — the Ultimate Spike Detox represents a reasonable, evidence-informed starting point. It is not a miracle cure, and results are gradual and variable. Careful physician involvement, particularly for patients on anticoagulants or with cardiovascular comorbidities, is essential. Serial spike protein antibody testing provides a practical objective marker of progress.
References
- 1. McCullough PA, Hrycak NE, Armstrong B. Clinical Approach to Post-acute Sequelae After COVID-19 Infection and Vaccination. Cureus. 2023 Nov 21;15(11):e49204. PMC10663976.
- 2. Preprints.org. 2023 Most Popular Preprints Award. preprints.org/activity/award/announcement.
- 3. Halma MTJ, Plothe C, Marik P, Lawrie TA. Strategies for the Management of Spike Protein-Related Pathology. Microorganisms. 2023;11(5):1308. Also: Autopsy Proven Fatal COVID-19 Vaccine-Induced Myocarditis. Eur J Heart Fail. doi:10.1002/ehf2.14680.
- 4. Tanikawa T, Kiba Y, Yu J, et al. Degradative Effect of Nattokinase on Spike Protein of SARS-CoV-2. Molecules. 2022 Aug 24;27(17):5405. PMID: 36080170; PMCID: PMC9458005.
- 5. PubMed nattokinase literature repository: pubmed.ncbi.nlm.nih.gov/?term=nattokinase (>250 indexed studies as of 2025).
- 6. Boschi D, Scheim DE, et al. SARS-CoV-2 Spike Protein Induces Hemagglutination: Implications for COVID-19 Morbidities and Therapeutics and for Vaccine Adverse Effects. Int J Mol Sci. 2022;23(24):15480. doi:10.3390/ijms232415480.
- 7. Stone S, et al. 62% Normalization in SpO2 within 24 Hours for Severe COVID-19 Patients after Ivermectin-Based Combination Treatment. Infect Dis Rep. 2022;2(3):15. doi:10.3390/idr2030015.
- 8. OneDayMD.com. Ivermectin and Fenbendazole: Treating Turbo Cancer. 2026.
- Comments should refer to the FAQ section for common clinical questions. The comments section is for general discussion; we cannot provide individual medical advice.
- While we do not ask for blind trust, our primary goal is to empower readers to conduct thorough research and make informed healthcare decisions in consultation with their trusted physician.
- Given the absence of completed clinical trials for post-acute COVID syndrome, recommendations in related protocols are based on known pathophysiological mechanisms and collective clinical experience of treating physicians.
- This protocol has also been applied to post-vaccine inflammatory syndromes with similar reported outcomes. Protocol components, doses, and durations will evolve as clinical data accumulates.


.png)







Comments
Post a Comment