Early Treatment Protocols for COVID-19: Early Treatment Can Reduce COVID-19 Hospitalizations and Deaths?
It is critical to recognize that infection with SARS-CoV-2, the virus that causes COVID-19, progresses through a number of stages and phases. Treatment is therefore highly stage-specific. COVID-19 is a clinical diagnosis; a confirmed antigen or PCR test is not required. Treatment should be initiated immediately after the onset of flu-like symptoms. The multiple therapies and drugs in this protocol have different mechanisms of action and work synergistically during various phases of the disease.

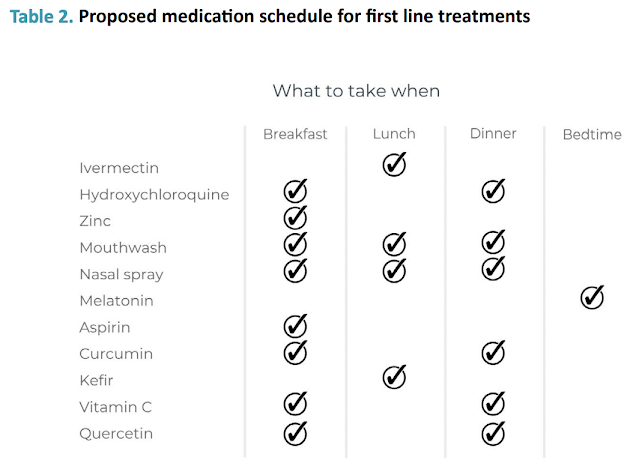
The FLCCC I-CARE Early Treatment Protocol
The I-Care protocol has been updated several times and below is their latest version (version 3: September 6, 2022).
FIRST LINE THERAPIES (In order of priority; not all required)- Ivermectin: 0.4 to 0.6 mg/kg – one dose daily for at least 5 days or until symptoms resolve. If symptoms persist longer than 5 days, consult a healthcare provider. See Table 1 for help with calculating correct dose. Due to a possible interaction between quercetin and ivermectin, these drugs should be staggered throughout the day (see Table 2). For COVID treatment, ivermectin is best taken with a meal or just following a meal, for greater absorption.
- Hydroxychloroquine (HCQ): 200 mg twice a day for 5 to 10 days. Best taken with zinc. HCQ may be taken in place of, or together with, ivermectin. While ivermectin should be avoided in pregnancy, the FDA considers HCQ safe in pregnancy. Given the pathway used by the Omicron variant to gain cell entry, HCQ may be the preferred drug for this variant.
- Zinc: 75-100 mg daily. Take with HCQ. Zinc supplements come in various forms (e.g., zinc sulfate, zinc citrate and zinc gluconate).
- Mouthwash: three times a day. Gargle three times a day (do not swallow) with an antiseptic-antimicrobial mouthwash containing chlorhexidine, cetylpyridinium chloride (e.g., Scope™, Act™, Crest™) or povidone-iodine (e.g. Betadine® Antiseptic Sore Throat Gargle™).
- Nasal spray with 1% povidone-iodine: 2-3 times a day. Do not use for more than 5 days in pregnancy. If 1% product is not available, dilute the more widely available 10% solution (see box) and apply 4-5 drops to each nostril every 4 hours.
- Aspirin: 325 mg daily (unless contraindicated).
- Melatonin: 5-10 mg before bedtime (causes drowsiness). Slow- or extended-release formulations preferred.
- Nigella sativa: If using seeds, take 80 mg/kg once a day (or 400 to 500 mg of encapsulated oil twice a day).
- Honey: 1 g/kg one to two times a day
- Kefir and/or Bifidobacterium Probiotics.
- Vitamin C: 500-1000 mg twice a day.
- Home pulse oximeter: Monitoring of oxygen saturation is recommended in symptomatic patients, due to asymptomatic hypoxia. Take multiple readings over the course of the day and regard any downward trend as ominous. Baseline or ambulatory desaturation under 94% should prompt consultation with primary or telehealth provider, or evaluation in an emergency room.
SECOND LINE THERAPIES (In order of priority/importance)
Add to first line therapies above if:
1) more than 5 days of symptoms;
2) poor response to first line agents;
3) significant comorbidities.
- Nitazoxanide (NTZ): 600 mg twice a day for 5 days.
- Curcumin (turmeric): 500 mg twice a day. Curcumin has low solubility in water and is poorly absorbed by the body; consequently, it is traditionally taken with full fat milk and black pepper, which enhance its absorption.
- Quercetin (or a mixed flavonoid supplement): 250 mg twice a day. Due to a possible interaction between quercetin and ivermectin, these drugs should not be taken simultaneously (i.e., should be staggered at different times of day – see Table 2). As supplemental quercetin has poor solubility and low oral absorption, lecithin-based and nanoparticle formulations are preferred.
- Vitamin D3: 10,000 IU daily (two 5,000 IU capsules) for two weeks.
- B complex vitamins.
- Fluvoxamine: 25-50 mg twice a day. Can substitute fluoxetine (Prozac; 20-40mg daily) if fluvoxamine not available.
- N-acetyl cysteine (NAC): 600-1200 mg orally twice a day.
- Omega-3 fatty acids: 4 g daily. Vascepa (Ethyl eicosapentaenoic acid); Lovaza (EPA/DHA); or alternative DHA/EPA. Vascepa and Lovaza tablets must be swallowed and cannot be crushed, dissolved, or chewed.
Table 1. How to calculate ivermectin dose

TREATMENT OF OMICRON BA.4/BA.5 VARIANT
The following protocol should be used where BA/4/BA.5 is the predominant circulating strain.
- Hydroxychloroquine: (200 mg twice daily or 400 mg daily for 5 days) AND Ivermectin (0.4-0.6 mg/kg once daily for 5 days taken with a fatty meal). Alternative to ivermectin: Nitazoxanide (500 mg three times a day for 5 days taken with a fatty meal).
- Zinc: (75-100 mg for 5 days).
- Antiseptic/antimicrobial mouthwash: (3 times daily).
- Nasal spray with 1% povidone-iodine: (2-3 times daily).
- Melatonin: (5-10 mg at night — slow-release formulation preferred).
- Nigella sativa: (seeds 80 mg/kg once a day or encapsulated oil 400-500 mg twice a day) taken with honey (1 g/kg one to two times a day).
- Aspirin: 325 mg daily unless contraindicated).
- Home pulse oximetry High-risk patients (aged over 60, comorbidities, poorly ambulatory), delayed treatment, high D-dimer, recently vaccinated, or severe symptoms, should add:
- Apixaban: (5 mg daily for 15 days) OR Rivaroxaban (10 mg daily for 15 days).
- Spironolactone: (200 mg once daily for 7 days — avoid in patients with impaired renal function). If symptoms have not markedly improved by day 3 of treatment, the following medications should be started. [NOTE: physicians should provide prescriptions for these medications at first visit.]
- Prednisolone: (60 mg daily for 5 days).
- Oral antibiotic: Doxycycline (100 mg twice daily for 5 days) (Doxycycline may act synergistically with ivermectin and may be the antibiotic of first choice) OR Azithromycin (Z-pack) (500 mg day 1, then 250 mg daily for 4 days) OR Amoxicillin/ Clavulanate (Augmentin) (500 mg/125 mg tablet twice daily for 7 days).
Ordinary Vitamin D3 Does not work in Acute Illness
According to this webinar (below) by Dr Pierre Kory and Dr. Keith Berkowitz:
Video time from 11:30 - 12:30:
Vitamin D3 (ordinary form) does not work in acute illness. It doesn't become active for at least a week... Vitamin D3 is for prevention and you should continue to take it if your levels are below 50 ng/ml...
There is only one form of vitamin D that will have an acute impact and that is calcifediol (vitamin D3 analog).
d.velop Vitamin D Supplements 2400 IU, 20 mcg – High Potency Vitamin D3
 |
| Check Price on Amazon |
Calcifediol, the form of vitamin D in d.velop, doesn’t need to be processed by the liver, it can be absorbed right into the bloodstream and throughout your body. That's why calcifediol is 3x more effective for raising vitamin D levels when compared to regular vitamin D on an equal microgram (mcg) basis.
Other FLCCC protocols
To find a list of physicians who follow the protocols and provide in-office and telehealth services: List of Doctors that will prescribe Ivermectin.
To find a list of pharmacist: List of Pharmacies that will fill Ivermectin.
COVID-19 is a highly dynamic topic. Please refer to the latest FLCCC I-CARE protocol (constantly updated).
The NIH COVID-19 Treatment Guidelines Panel’s Statement on Early Therapies for Nonhospitalized Adults With COVID-19 (Last Updated: September 26, 2022)
This statement contains the Panel’s recommendations for treating these non-hospitalized patients using the currently available therapies.
The Panel’s recommendations take into account the efficacies of these drugs and the high prevalence of the Omicron VOC. When resources are limited, therapy should be prioritized for patients who are at the highest risk of progressing to severe COVID-19.
For All Patients:
- All patients should be offered symptom management.
- The Panel recommends against the use of dexamethasonea or other systemic corticosteroids in the absence of another indication.
The Panel’s current outpatient treatment recommendations are as follows (in order of preference):
Preferred Therapies
- Paxlovid (Ritonavir-boosted nirmatrelvir )
- Remdesivir
Alternative Therapies
For use only when neither of the preferred therapies are available, feasible to use, or clinically appropriate. Listed in alphabetical order:
- Bebtelovimab (monoclonal antibody from Eli Lilly)
- Molnupiravir
- Bebtelovimab is active in vitro against circulating Omicron subvariants, but there are no clinical efficacy data from placebo-controlled trials that evaluated the use of bebtelovimab in patients who are at high risk of progressing to severe COVID-19. Therefore, bebtelovimab should be used only when the preferred treatment options are not available, feasible to use, or clinically appropriate.
For post-covid or long covid syndrome, check out Long Haulers Treatment Protocol.
Disclaimers: Please do not consider these protocols as personal medical advice, but as a recommendation for use by professional providers. Consult with your doctor, share the information on this website and discuss with her/him.

.png)








Comments
Post a Comment