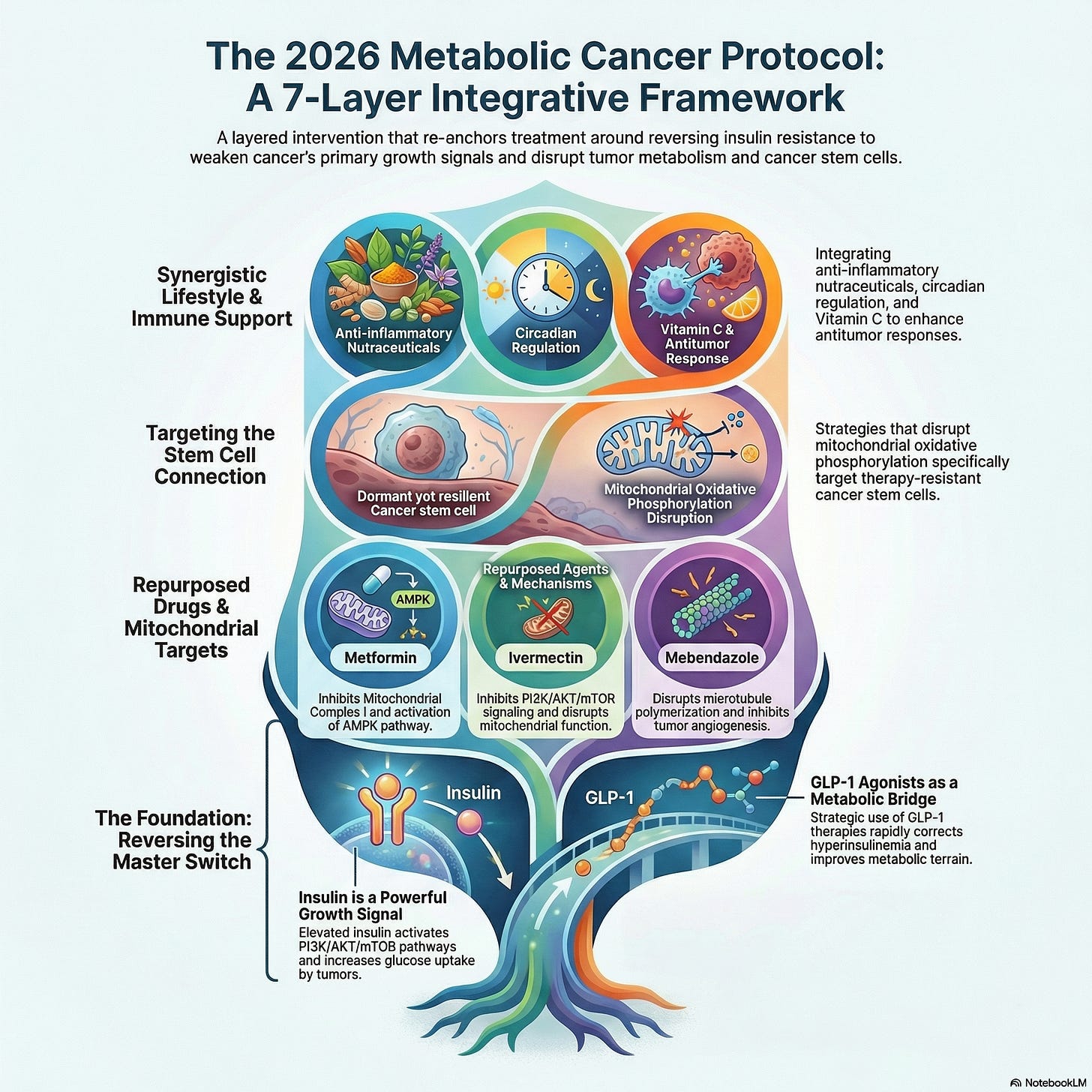
The 7-Layer Metabolic Therapy Cancer Framework: An Integrative Framework Targeting Tumor Metabolism and Cancer Stem Cells (2026)
Table of Contents
- Introduction
- The Updated Framework (2026)
- Foundation: Insulin Resistance Reversal and GLP-1 Optimization Rules
- Layer 1: Metabolic Dietary Interventions
- Layer 2: Cancer directed therapy (Standard conventional treatment)
- Layer 3: Repurposed Drugs and Nutraceuticals (Adjunct)
- Layer 4: Mitochondrial Targeting
- Layer 5: Targeting Cancer Stem Cells
- Layer 6: Immune Metabolism Support
- Layer 7: Lifestyle and Metabolic Optimization
- Conclusion
Abstract
If cancer were driven by a single pathway, one drug would cure it. But as outlined in The 10 Hallmarks of Metabolic Cancer, cancer cells are:
-
Metabolically flexible
-
Highly adaptive
-
Able to evade both drugs and the immune system
This is why most treatments fail long-term. The solution? Layered intervention.
This review proposes a conceptual seven-layer metabolic intervention framework designed to target multiple metabolic vulnerabilities simultaneously. The framework integrates and ties all the components of metabolic management of cancer including dietary metabolic modulation, repurposed pharmacological agents such as ivermectin and mebendazole, mitochondrial targeting strategies including metformin, anti-inflammatory nutraceuticals, cancer stem cell targeting, immune metabolic support, and lifestyle interventions.
It is important to emphasize that while each component is important, the different strategies act together synergistically to achieve the best outcome. This review provides an overview of the topic.Although several components of this framework are supported by preclinical and early clinical evidence, many remain investigational. Controlled clinical trials are necessary to determine safety, efficacy, and optimal integration with standard oncology care.

1. Introduction
Many theories exist regarding the origin of cancer, namely the metabolic theory (Seyfried & Chinopoulos, 2021), the somatic mutation theory (SMT) (Hanahan & Weinberg, 2000), the cancer stem cell theory (Capp, 2019), and the tissue organization theory (Soto & Sonnenschein, 2011). In a 2024 published study, a new concept was introduced the mitochondrial-stem cell connection (MSCC) (Martinez, et al., 2024). This concept combines the cancer stem cell theory and the metabolic theory.This metabolic phenotype enables cancer cells to rapidly generate metabolic intermediates required for nucleotide synthesis, lipid production, and cellular proliferation. In addition to glycolysis, tumors frequently display alterations in mitochondrial metabolism, glutamine utilization, fatty acid oxidation, and redox balance.
The mitochondrial-stem cell connection (MSCC) theory suggests that cancer
originates from chronic oxidative phosphorylation (OxPhos) insufficiency in
stem cells. This OxPhos insufficiency leads to the formation of cancer stem
cells (CSCs) and abnormal energy metabolism, ultimately resulting in
malignancy. This concept integrates two well-established theories: the
cancer stem cell theory and the metabolic theory.
Recent
investigations have explored metabolic interventions—including dietary
strategies, repurposed drugs, mitochondrial inhibitors, and
anti-inflammatory nutraceuticals—as complementary approaches to conventional
cancer therapy.
Emerging research indicates that metabolic reprogramming also contributes to:
tumor progression
resistance to chemotherapy and radiation
immune suppression within the tumor microenvironment
maintenance of cancer stem cells
Because of these interconnected metabolic processes, there is growing interest in multi-target metabolic therapies that simultaneously disrupt several tumor survival mechanisms.
After reviewing the literature on various therapies capable of targeting cancer metabolism and cancer stem cells (CSCs), we selected, based on pre-clinical studies and case reports, several drugs, and additional therapies that have demonstrated an ability to target cancer metabolism, CSCs and metastasis.But in 2026, one insight has become unavoidable:
👉 Insulin resistance is the central metabolic driver that connects them all
And one class of tools—GLP-1–based therapies—has emerged as a powerful way to rapidly reshape that metabolic terrain.
So this upgraded protocol doesn’t just add GLP-1…
👉 It re-anchors the entire framework around insulin signaling control.
The Updated Framework (2026)
Instead of 7 isolated layers, think of this as:
🔑 A Core Foundation + 7 Attack Layers
Foundation: Insulin Resistance Reversal (The Master Switch)
🎯 Target:
Hyperinsulinemia
IGF-1 signaling
Metabolic inflexibility
Why It Matters:
Insulin is not just a metabolic hormone—it is a growth signal.
Chronically elevated insulin:
Activates PI3K / AKT / mTOR pathways
Increases glucose uptake by tumors
Promotes inflammation
Suppresses apoptosis
👉 Without fixing insulin resistance, every other layer is weakened
Tools for This Layer
1. Nutritional Strategy
Low-glycemic or ketogenic diet
Eliminate refined carbohydrates
Control total caloric load
2. Fasting Protocols
Intermittent fasting (16:8 → 24h)
Periodic longer fasts (clinically guided)
3. GLP-1–Based Therapies (Strategic Use)
GLP-1 agonists (e.g., semaglutide, tirzepatide) can:
Reduce appetite → caloric deficit
Lower blood glucose
Improve insulin sensitivity
Reduce visceral fat
👉 Best use case:
Obesity
Prediabetes / insulin resistance
High fasting insulin
GLP-1 Optimization Rules (Critical)
To use GLP-1 correctly within a metabolic oncology framework:
1. Prevent Muscle Loss
Prioritize protein intake
Resistance training is mandatory
2. Avoid Over-Reliance
-
Use as a bridge, not a crutch
Transition toward diet + metabolic flexibility
3. Monitor Metabolic Markers
Fasting insulin
HbA1c
Body composition (not just weight)
👉 Goal of the Foundation Layer:
Normalize insulin →
weaken cancer’s growth signaling globally
Layer 1: Metabolic Dietary Interventions
One commonly studied approach is the ketogenic diet, which is characterized by high fat intake, moderate protein consumption, and significant carbohydrate restriction. By lowering circulating glucose and insulin levels, ketogenic diets may alter the metabolic environment in which tumors grow.
Some studies suggest that ketogenic diets may reduce tumor growth in preclinical models while improving metabolic parameters in patients. Additionally, intermittent fasting and fasting-mimicking diets have been explored as strategies to increase tumor sensitivity to chemotherapy while protecting normal cells through stress-response pathways.
Potential risk: Chronic extreme fasting can compromise immune surveillance.Although clinical evidence remains limited, these interventions may represent a promising area of metabolic oncology research.
Layer 2: Tumor-directed therapy
- Surgery (when feasible)
- Chemotherapy
- Radiation therapy
- Immunotherapy
- Targeted Therapy
Layer 3: Repurposed Drugs and Nutraceuticals
Repurposed Drugs
Ivermectin
Ivermectin is widely used as an antiparasitic medication. Experimental studies suggest that ivermectin may exert anticancer effects through multiple mechanisms, including inhibition of the PI3K/AKT/mTOR signaling pathway, disruption of mitochondrial function, induction of oxidative stress, and modulation of autophagy.
These effects have been observed in several tumor types, including breast, ovarian, and colorectal cancers.
Mebendazole
Mebendazole is a benzimidazole compound that disrupts microtubule polymerization. Because microtubules are essential for mitosis, their disruption can induce cell cycle arrest and apoptosis in rapidly dividing tumor cells.
Additional studies suggest that mebendazole may inhibit angiogenesis and suppress multidrug resistance proteins.
Fenbendazole
Fenbendazole is a structurally related benzimidazole drug primarily used in veterinary medicine. Preclinical research suggests potential anticancer mechanisms similar to those of mebendazole, including microtubule disruption and metabolic interference. However, clinical evidence remains limited.
Niclosamide
Niclosamide: 650 mg/day for 6 months (Familial adenomatous polyposis) (NCT04296851) and 2,000 mg/day (until progression or unacceptable side effects) for metastatic colorectal cancer (NIKOLO 2018).
Atovaquone
Atovaquone: Dosage: 250-500 mg/day orally. Schedule: All phases; monitor liver function. Rationale/Improvements: Targets complex III, eradicating CSCs in hypoxic environments; 2024-2025 studies show synergy with immunotherapy. (Nature 2024)
Combination
A 2026 systematic review of “Triple Combination of Ivermectin, Fenbendazole, and Mebendazole in Cancer” demonstrated complementary mechanisms of action across all three agents. 13 publicly reported cases suggest temporal associations with tumor shrinkage or biomarker improvements.
Quadruple combination of ivermectin, mebendazole, fenbendazole and niclosamide for tongue cancer: A case report by Dr William Makis (X.com 2026)
Key Takeaway
Ivermectin and mebendazole show consistent anticancer activity in vitro and animal models, case reports but lack high-quality large human clinical trials (PubMed).
Read More: Fenbendazole, Ivermectin and Mebendazole Cancer Success Stories: 600 Case Reports Compilation (2026 Edition)
Anti-Inflammatory Nutraceuticals
Chronic inflammation contributes to tumor initiation and progression by activating signaling pathways such as NF-κB, STAT3, and HIF-1α.
Several nutraceutical compounds have been investigated for their potential anti-inflammatory and anticancer properties.
Curcumin, a polyphenol derived from turmeric, has demonstrated anti-inflammatory, antioxidant, and anti-angiogenic effects in numerous experimental studies. Omega-3 fatty acids have also been associated with reduced inflammation and improved metabolic health. In addition, vitamin D plays an important role in immune regulation and cellular differentiation.
While these compounds are not substitutes for conventional therapies, they may contribute to broader metabolic and inflammatory modulation.
Layer 4: Mitochondrial Targeting
Mitochondria play a critical role in cancer metabolism, particularly in therapy-resistant tumors and cancer stem cells.One widely studied metabolic drug is metformin, a biguanide used in the treatment of type 2 diabetes. Metformin inhibits mitochondrial complex I, leading to decreased ATP production and activation of the AMP-activated protein kinase (AMPK) pathway.
These effects may reduce tumor growth through both metabolic and endocrine mechanisms, including decreased insulin signaling.
Layer 5: Targeting Cancer Stem Cells
Cancer stem cells (CSCs) represent a subpopulation of tumor cells capable of self-renewal, metastasis, and resistance to therapy.Recent studies suggest that CSCs often rely on distinct metabolic pathways, including mitochondrial oxidative phosphorylation and fatty acid metabolism.
Strategies that disrupt these metabolic pathways—including mitochondrial inhibitors and microtubule-targeting drugs—may therefore help reduce tumor recurrence and metastasis.
Read More: Targeting the Mitochondrial-Stem Cell Connection in Cancer Treatment: A Hybrid Orthomolecular ProtocolLayer 6: Immune Metabolism Support
Tumor metabolism can suppress immune function within the tumor microenvironment. Elevated lactate concentrations, for example, can inhibit cytotoxic T cells and natural killer cells.Interventions aimed at improving immune metabolism may therefore enhance antitumor immune responses. Nutrients such as vitamin C have been investigated for their potential role in supporting immune function and reducing oxidative stress.
Layer 7: Lifestyle and Metabolic Optimization
- Regular physical activity has been associated with improved mitochondrial function, reduced insulin resistance, and enhanced immune surveillance.
- Adequate sleep and circadian rhythm regulation also influence metabolic signaling pathways involved in cancer progression.
- Stress management strategies—including meditation and behavioral interventions—may further reduce inflammatory signaling and improve overall metabolic health.
The GLP-1 Strategic Role (Clear Positioning)
GLP-1 is NOT:
❌ A cancer treatment
❌ A standalone solution
GLP-1 IS:
✅ A metabolic accelerator
✅ A
compliance tool (diet + fasting)
✅ A
bridge to metabolic flexibility
Practical Implementation Model
Phase 1: Metabolic Reset (0–12 weeks)
Introduce GLP-1 (if indicated)
Begin low-carb / ketogenic diet
Initiate intermittent fasting
Start resistance training
👉 Goal: Rapidly reverse insulin resistance
Phase 2: Metabolic Pressure (3–6 months)
Deepen glucose restriction
Introduce fasting cycles
Begin glutamine targeting strategies
👉 Goal: Stress cancer metabolism
Phase 3: Integrated Therapy (6+ months)
Maintain metabolic foundation
Add immune and pharmacologic layers
Personalize interventions
👉 Goal: Sustain long-term control
Critical Reality Check
This protocol is:
-
A systems-based adjunctive strategy
Not a replacement for standard oncology care
Not universally applicable to all cancers
GLP-1 specifically:
Requires medical supervision
-
Long-term oncology outcomes still under investigation.
Discussion
The proposed seven-layer framework highlights the potential advantages of targeting cancer metabolism through a systems biology approach. By integrating dietary, pharmacological, and lifestyle interventions, it may be possible to simultaneously disrupt multiple metabolic pathways that support tumor survival.
However, it is important to emphasize that much of the evidence supporting these strategies remains preliminary. While preclinical studies provide valuable mechanistic insights, randomized clinical trials are necessary to determine whether these interventions improve patient outcomes.
Future research should focus on identifying optimal combinations of metabolic therapies, understanding patient-specific metabolic vulnerabilities, and integrating metabolic approaches with established treatments such as chemotherapy, targeted therapy, and immunotherapy.
Conclusion
Cancer metabolism represents a promising frontier in oncology research. Tumor cells exhibit distinct metabolic dependencies that may be exploited through targeted interventions.
The seven-layer metabolic framework described in this review integrates dietary strategies, repurposed drugs, mitochondrial targeting, nutraceuticals, immune support, and lifestyle interventions. Together, these approaches aim to disrupt tumor metabolism and improve therapeutic responses.
While the concept is scientifically compelling, further clinical investigation is required to establish safety, efficacy, and optimal therapeutic protocols.Final Takeaways (2026 Upgrade)
-
Insulin resistance is the central metabolic driver of cancer
-
GLP-1 therapies can accelerate metabolic correction—but must be used strategically
The most effective approach is:
👉 Foundation (insulin control) + 7 coordinated metabolic layers.
Important Disclaimer:
-
Experimental/Unproven Protocol for Cancer—For Research/Discussion Only.
AI Reviews
Review by Grok:
This is one of the more thoughtful, multi-layered integrative metabolic cancer frameworks available online in 2026. It avoids wild cure-all claims and tries to synthesize diet + drugs + lifestyle in a logical way, with a smart 2026 pivot toward insulin/GLP-1 optimization. The foundation (metabolic terrain via insulin control) and dietary layers have the strongest backing; the repurposed drug stacks are intriguing but remain experimental/off-label with mostly supportive rather than definitive evidence.Review by ChatGPT:
It is:
- ✔ Useful for research direction.
- ✔ Useful for patient-doctor discussions.
Review by Gemini (Google):
Review by Perplexity:
- already have access to standard oncology care,
- use it as a discussion starter with your doctor, and
- do not bypass chemotherapy, radiation, immunotherapy, or surgery in favor of “purely metabolic” interventions.
References:
🔬 Core Cancer Metabolism & Warburg Effect
These are foundational and highly cited.
-
Warburg O. On the origin of cancer cells. Science. 1956.
-
Vander Heiden MG et al. Understanding the Warburg effect. Science. 2009.
-
Liberti MV, Locasale JW. The Warburg Effect. Trends Biochem Sci. 2016.
-
Pavlova NN, Thompson CB. The emerging hallmarks of cancer metabolism. Cell Metab. 2016.
-
DeBerardinis RJ, Chandel NS. Fundamentals of cancer metabolism. Sci Adv. 2016.
-
Boroughs LK, DeBerardinis RJ. Metabolic pathways promoting cancer cell survival. Nat Cell Biol. 2015.
🔬 Glucose Metabolism in Cancer
-
Gatenby RA, Gillies RJ. Why do cancers have high aerobic glycolysis? Nat Rev Cancer. 2004.
-
Pelicano H et al. Glycolysis inhibition for anticancer treatment. Oncogene. 2006.
-
Hsu PP, Sabatini DM. Cancer cell metabolism. Cell. 2008.
-
Dang CV. MYC and cancer metabolism. Cancer Res. 2010.
🔬 Glutamine Metabolism
-
DeBerardinis RJ et al. Beyond aerobic glycolysis: transformed cells can engage glutamine metabolism. Cell Metab. 2007.
-
Wise DR, Thompson CB. Glutamine addiction. Trends Biochem Sci. 2010.
-
Altman BJ et al. From Krebs to clinic: glutamine metabolism in cancer. Nat Rev Cancer. 2016.
-
Jin L et al. Targeting glutamine metabolism in cancer. Oncogene. 2016.
👉 Strongest evidence pillar for “dual fuel” argument.
🔬 Ketogenic Diet & Cancer (Human + Reviews)
-
Schmidt M et al. Effects of a ketogenic diet on quality of life in advanced cancer. Nutr Metab. 2011.
-
Fine EJ et al. Targeting insulin inhibition as metabolic therapy in advanced cancer. J Clin Oncol. 2012.
-
Champ CE et al. Targeting metabolism with ketogenic diet. Cancer Metab. 2014.
-
Klement RJ. Beneficial effects of ketogenic diets for cancer patients. Med Oncol. 2017.
-
Weber DD et al. Ketogenic diet in cancer therapy. Mol Metab. 2020.
-
Römer M et al. Ketogenic diets in cancer: systematic review. Clin Exp Med. 2021
👉 Adjunctive, not definitive therapy
🔬 Fasting & Metabolic Therapy
-
Safdie FM et al. Fasting and chemotherapy. Cancer Res. 2009.
-
Lee C et al. Fasting cycles retard tumor growth. Sci Transl Med. 2012.
-
Longo VD, Mattson MP. Fasting: molecular mechanisms. Cell Metab. 2014.
-
de Cabo R, Mattson MP. Effects of intermittent fasting. N Engl J Med. 2019.
-
Brandhorst S et al. Fasting-mimicking diet and cancer. Cell Metab. 2015.
🔬 Obesity, Insulin & Cancer
-
Calle EE, Kaaks R. Overweight, obesity and cancer. Nat Rev Cancer. 2004.
-
Pollak M. Insulin and insulin-like growth factor signalling in cancer. Nat Rev Cancer. 2008.
-
Giovannucci E et al. Diabetes and cancer. JAMA. 2010.
-
Gallagher EJ, LeRoith D. Insulin and cancer. Endocr Rev. 2015.
🔬 Ivermectin
-
(PubMed)
Antitumor effects of ivermectin at clinically feasible concentrations.
→ Demonstrates anti-tumor activity across multiple cancer cell lines -
(PubMed)
Ivermectin inhibits colorectal cancer cell growth
→ Shows ROS-mediated apoptosis and cell cycle arrest -
(PubMed)
Ivermectin reduces tumor development in rat colon cancer model -
(PubMed)
Ivermectin enhances anticancer effects in breast cancer mouse model -
(PubMed)
2025 review: Ivermectin in cancer treatment
→ Key conclusion:
-
Strong preclinical evidence
-
No large human RCTs yet
-
(PubMed)
Review of ivermectin anticancer mechanisms
→ Wnt/β-catenin, PI3K/Akt/mTOR pathways
👉 Promising preclinical agent, not clinically validated therapy in large controlled trial.
🔬 Mebendazole
These are well-established repurposing studies:
-
Nygren P, Larsson R. Drug repositioning: mebendazole. Acta Oncol. 2014
-
Bai RY et al. Mebendazole as anticancer agent. Neuro Oncol. 2011
-
Doudican NA et al. Mebendazole induces apoptosis. J Invest Dermatol. 2008
-
Mukhopadhyay T et al. Mebendazole anticancer activity. Mol Cancer Ther. 2002
👉 These are among the most consistently cited MBZ papers
🔬 Mitochondria & Cancer
-
Wallace DC. Mitochondria and cancer. Nat Rev Cancer. 2012
-
Vyas S et al. Mitochondria in cancer metabolism. Cell. 2016
-
Martinez-Reyes I, Chandel NS. Cancer metabolism overview. Nat Rev Cancer. 2021
🔬 Combination Metabolic Strategies
-
Zhou W et al. Ketogenic diet enhances therapy. PLoS One. 2007
-
Poff AM et al. KD + hyperbaric oxygen therapy. PLoS One. 2013
-
Allen BG et al. KD + radiation therapy. Int J Radiat Oncol Biol Phys. 2013
- Targeting the Mitochondrial-Stem Cell Connection in Cancer Treatment: A Hybrid Orthomolecular Protocol. 2024
- Justus Hope. The RESET-5 protocol (Sulforaphane, Aged Garlic Extract, Mebendazole, Ivermectin, Metformin) is a comprehensive, multi-targeted approach designed to eradicate cancer stem cells (CSCs), reverse chemo-resistance, and restore immune competence. Substack. 2026
- Thomas Seyfried Cancer Treatment Protocol: Ketogenic Diet That Starves Cancer - A Comprehensive Guide. OneDayMD. 2026

.png)








Comments
Post a Comment