PolyPill SECURE Trial Review: Dr Chris Centeno
It’s been a while since I’ve blogged on the highly profitable world of cholesterol meds, which in my opinion, is a great example of big pharma malfeasance. Remember that scene in The Godfather: Part 3 when Michael Corleone exclaims, “Just when I thought I was out, they pull me back in,” so it was with a national news story involving “polypills” and WHO. Let’s dig in.
The News Story
This story appeared on my morning news feed: “Heart drug combining 3 medications in one is added to World Health Organization’s list of essential medicines”. The gist of this report was that the WHO added the “Polypill” which contains a statin, aspirin, and an ACE inhibitor blood pressure medicine, to its list of approved medications. This is a big deal, given that this means that many developing countries will now add purchasing Polypills to their national health strategies. This was based on this quote from the story gleaned from a press release put out by Mount Sinai:
“The polypill also reduced cardiovascular mortality by 33% among patients who had previous heart attacks, the study found.”
Wow, that certainly sounds like a huge deal. However, let’s look a bit deeper.
Relative vs. Absolute Risk
From reading the story and Mount Sinai press release, you would think the Polypill reduced mortality from 40% to 7% (33% less), which would be a very BIG DEAL. However, from looking at the actual study that was being quoted, that’s not what happened (1):
“A total of 2499 patients underwent randomization and were followed for a median of 36 months. A primary-outcome event occurred in 118 of 1237 patients (9.5%) in the polypill group and in 156 of 1229 (12.7%) in the usual-care group (hazard ratio, 0.76; 95% confidence interval [CI], 0.60 to 0.96; P = 0.02).”
What actually happened was that during a 3-year period, 9.5% of the Polypill group had a cardiovascular death, nonfatal type 1 myocardial infarction, nonfatal ischemic stroke, or urgent revascularization, and 12.7% of the control group had the same event. Hence the absolute risk reduction for that outcome was 3.2%! Since this was over three years, 1% of the people with a prior heart attack annually didn’t have an event by taking the Polypill.
However, it gets much worse from there. When just looking at the outcome of “Cardiovascular Death,” the results were less robust, with 3.9% dying this way in the polypill group vs. 5.8% in the control group, or a 1.9% absolute risk reduction. That’s a 0.6% annual reduction in that outcome.
Those outcomes are lackluster at best and barely measurable at worst. This is the kind of drug study result that has minimal benefit for any given patient and only makes sense if we’re talking about medicating large groups. On that front, we then see this bomb of a statement in the paper:
“The incidence of death from any cause was similar in the two groups. Although there was no substantial between-group difference in the incidence of death from noncardiovascular causes, more cases were observed in the polypill group than in the usual-care group, driven mainly by cancer deaths (21 in the polypill group vs. 11 in the usual-care group).”
The authors attempted to explain this higher cancer death rate among Polypill users by stating that the Polypill was so effective that the much lower number of cardiac-related deaths left more people open to cancer death. However, as you can see, the Polypill impact on cardiac death was a measly 1.9% over three years, so that’s more spin than reality.
33% Risk Reduction?
So where in the world did they get a 33% risk reduction? Through this math:
3.9% Polypill Cardiac Death/5.8% Control Cardiac Death=0.67
1-0 – 0.67=0.33
0.33 X 100=33%
So the authors took a barely-there effect of a 1.9% absolute reduction in cardiac mortality over three years and converted it to a 33% relative risk reduction. They, of course, ignored that the overall risk of dying wasn’t reduced at all from the Polypill as more cancer deaths occurred in that group.
Could Statins Cause Cancer?
The Polypill has three ingredients, with two of these being prescription drugs: atorvastatin and the ACE inhibitor ramipril. Can statin cholesterol drugs like atorvastatin cause cancer? This is from a paper on that topic (2):
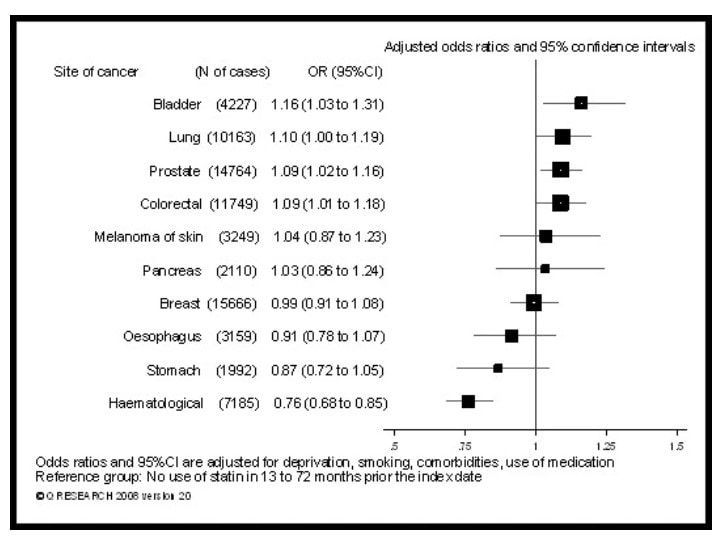
Statins increased the risk for six of the most common cancer types and reduced it in three of the common types of cancer.
How about the ACE inhibitor blood pressure drug in the Polypill? In one study, these drugs increased the risk of lung cancer by about 20% (3). This may be important here as 55% of the people in this study were smokers.
Hence it’s plausible that the increased cancer rate observed in this study was due to the Polypill. It should be noted that the authors quoted none of these studies.
The Authors
Here are the conflicts of interest disclosed by the authors:
- Deepak Bhatt: Almost 100 pharma companies disclosed that have funded this author (I honestly stopped counting after the first few dozen companies, and I wasn’t yet out of the “C”s in the alphabetized list).
- Yannick Bejot: 7 pharma company conflicts.
- Jose Castellano: 4 pharma company conflicts, including the maker of the tested Polypill.
- Wolfram Doehner: 4 pharma company conflicts.
- Franciso Marin: 1 pharma company conflict.
- Béla Merkely: 7 pharma company conflicts.
- Piotr Ponikowski: 12 pharma company conflicts.
- Francois Schiele: 6 pharma company conflicts.
- Tabassome Simon: 4 pharma company conflicts.
To say that a good chunk of these researchers are not naive to money and grants coming from pharma is an understatement.
This Is Not New
Here are my past blogs that also relate similar barely there absolute risk reductions for statin drugs and the relative risk reduction game played by pharma:
- Statins and Stem Cells: Barely There Results
- Statins Are More Business than Medicine
- Can We Stop the Fiction that Statins Are a Key Heart Disease Prevention Strategy?
- Blueberries or Statins to Reduce Heart Attack Risk? Your Call…
The upshot? Should the WHO have added the Polypill to its list of approved medicines? Not based on the data reported in the NEJM that I reviewed today. Basically, there was no change in all-cause mortality, which is a ridiculous result.
_______________________________________________________
References:
(1) Castellano JM, Pocock SJ, Bhatt DL, Quesada AJ, Owen R, Fernandez-Ortiz A, Sanchez PL, Marin Ortuño F, Vazquez Rodriguez JM, Domingo-Fernández A, Lozano I, Roncaglioni MC, Baviera M, Foresta A, Ojeda-Fernandez L, Colivicchi F, Di Fusco SA, Doehner W, Meyer A, Schiele F, Ecarnot F, Linhart A, Lubanda JC, Barczi G, Merkely B, Ponikowski P, Kasprzak M, Fernandez Alvira JM, Andres V, Bueno H, Collier T, Van de Werf F, Perel P, Rodriguez-Manero M, Alonso Garcia A, Proietti M, Schoos MM, Simon T, Fernandez Ferro J, Lopez N, Beghi E, Bejot Y, Vivas D, Cordero A, Ibañez B, Fuster V; SECURE Investigators. Polypill Strategy in Secondary Cardiovascular Prevention. N Engl J Med. 2022 Sep 15;387(11):967-977. doi: 10.1056/NEJMoa2208275. Epub 2022 Aug 26. PMID: 36018037.
(2) Vinogradova, Y., Coupland, C. & Hippisley-Cox, J. Exposure to statins and risk of common cancers: a series of nested case-control studies. BMC Cancer 11, 409 (2011). https://doi.org/10.1186/1471-2407-11-409
(3) Wu, Z., Yao, T., Wang, Z. et al. Association between angiotensin-converting enzyme inhibitors and the risk of lung cancer: a systematic review and meta-analysis. Br J Cancer 128, 168–176 (2023). https://doi.org/10.1038/s41416-022-02029-5
About the Author: Chris Centeno, MD is a specialist in regenerative medicine and the new field of Interventional Orthopedics. Centeno pioneered orthopedic stem cell procedures in 2005 and is responsible for a large amount of the published research on stem cell use for orthopedic applications.
Comments
Post a Comment