Large PRP Saline Control Study: a Comparison to Bennell et al
Chris Centeno, MD - What’s amazing is that every month now, we’re seeing new Platelet-Rich Plasma (PRP) studies coming out. A new one is interesting as it’s larger than the new JAMA study that was reported to be the “last word” on PRP and Knee Arthritis. So let’s dive into that comparison this morning.
The Benell et al and JAMA Epic Fail
I’ve already blogged on the recent JAMA study out of Australia that seemed to show that PRP when used to treat knee arthritis didn’t work (1). That paper showed different results than three dozen Randomized Controlled Trials that demonstrated that PRP was effective. Based on that stark difference, many looked more closely at the new JAMA paper and found:
- They never actually used PRP, but instead a product that could only achieve about a 1.6 X concentration of platelets. This is despite the minimum definition of PRP being 2X and up.
- The authors claimed to have concentrated the growth factors in their “PRP” but instead never measured the baselines amounts of these factors.
- The lead author of the paper is a seriously conflicted scientist who is involved in many different Osteoarthritis drugs that would compete with PRP in the marketplace.
Given that the vaunted journal JAMA and its reviewers never noted that the authors didn’t use PRP and their blood analysis shenanigans, many in the Orthobiologics community rolled their eyes.
The New Chu Saline Control RCT

While we have at least 6 RCTs showing that PRP when used to treat Knee Osteoarthritis beats a saline placebo (see above), a 7th just showed up and it studied a massive number of patients (2):
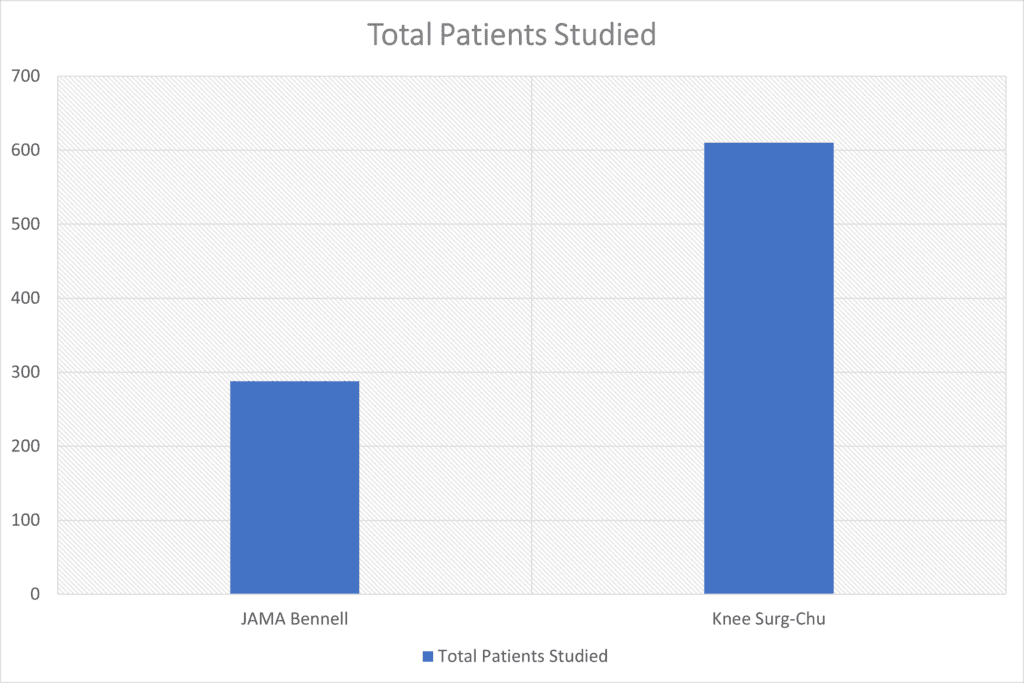
As shown above, the new Chu paper contains the results from over twice the number of patients than the JAMA Benell paper studied. If we look at the results between these two studies, there’s a marked difference:
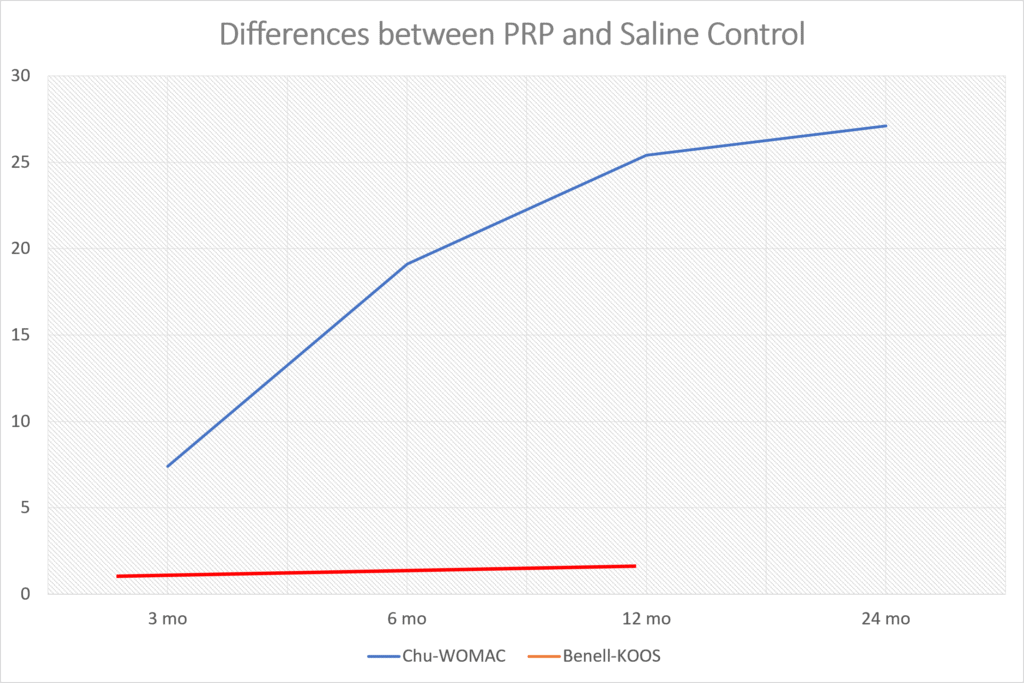
This graph was created by taking the average KOOS change in subscales from Bennell et al and then the average reported change in total WOMAC score for the Chu paper. More is better here, so you can see the Chu study showed a nice difference between the groups while Bennell et al didn’t. Could there be a reason?
Fake PRP vs. Real PRP
The main criticism of the Bennell et al paper is that they didn’t use PRP based on reporting a platelet count for their samples that was within the normal range of platelets in whole blood. When we compare the platelet counts in the PRP between the two studies we see this direct comparison:
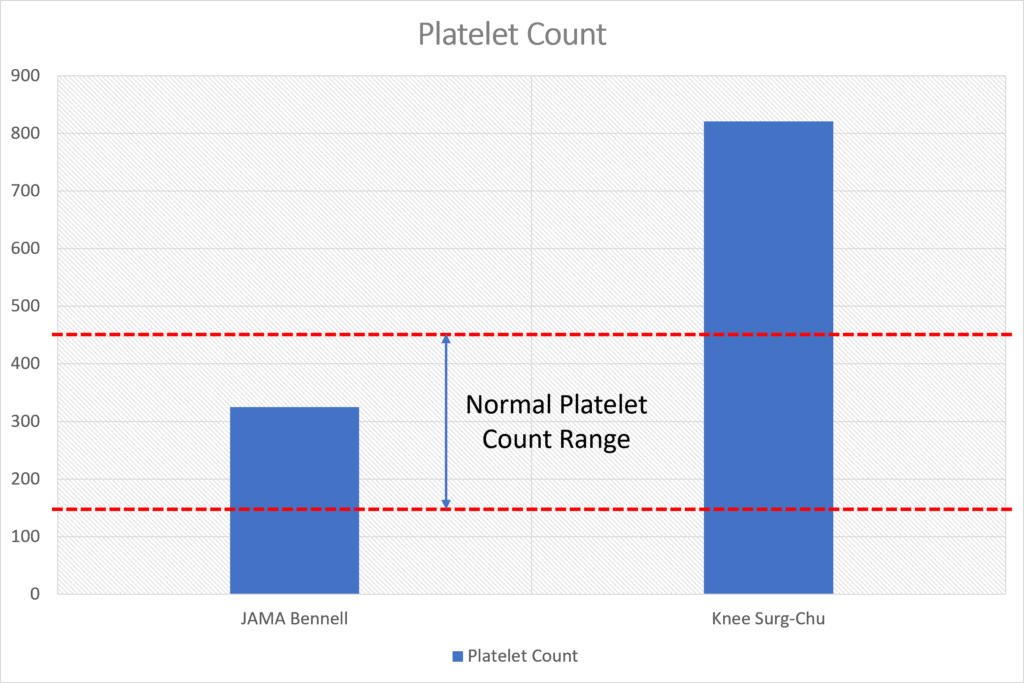
It doesn’t take a rocket scientist to figure out that the Chu study injected many more platelets into each knee. Given that the average platelet count in whole blood ranges from 150 to 450, you can see that Chu definitely concentrated platelets. How much did they concentrate their PRP? Check out this comparison graph:
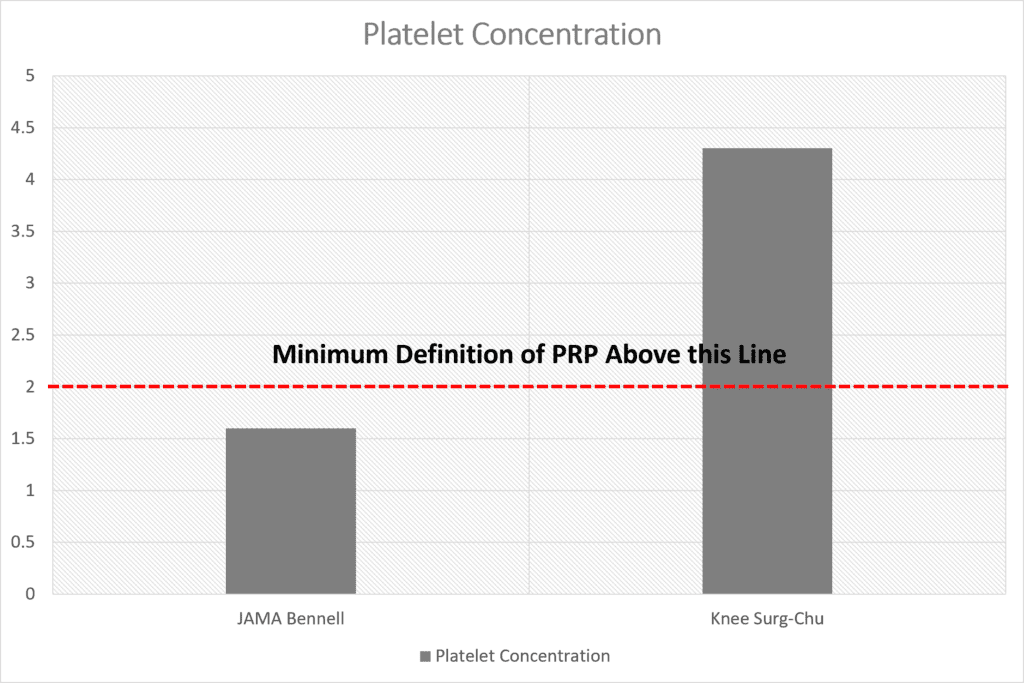
For the Bennell study, they never reported their baseline platelet levels, an omission which should have flagged it at JAMA as not being worthy of publication. However, they did report which system they used and the manufacturer’s reported data and we also know what independent studies of that system have shown (3). On the other hand, Chu et al did report their platelet numbers before and after, so we know that while Bennell likely only concentrated platelets at 1.6X, Chu et al concentrated platelets at more than 4X.
Platelet Concentration in PRP Matters!
We know from other clinical studies that platelet concentration is directly related to results (4). Meaning the more concentrated the PRP, the better the results in knee arthritis patients. Hence, it’s not surprising to see why the Chu et al study results are much better than Bennell et al.
This brings up a critical point for any patient wishing to have their knee arthritis treated with PRP. You need to make sure the doctor knows the concentration factor of platelets being injected. If it’s below 2X, that’s a problem. Which systems out there produce below 2X?
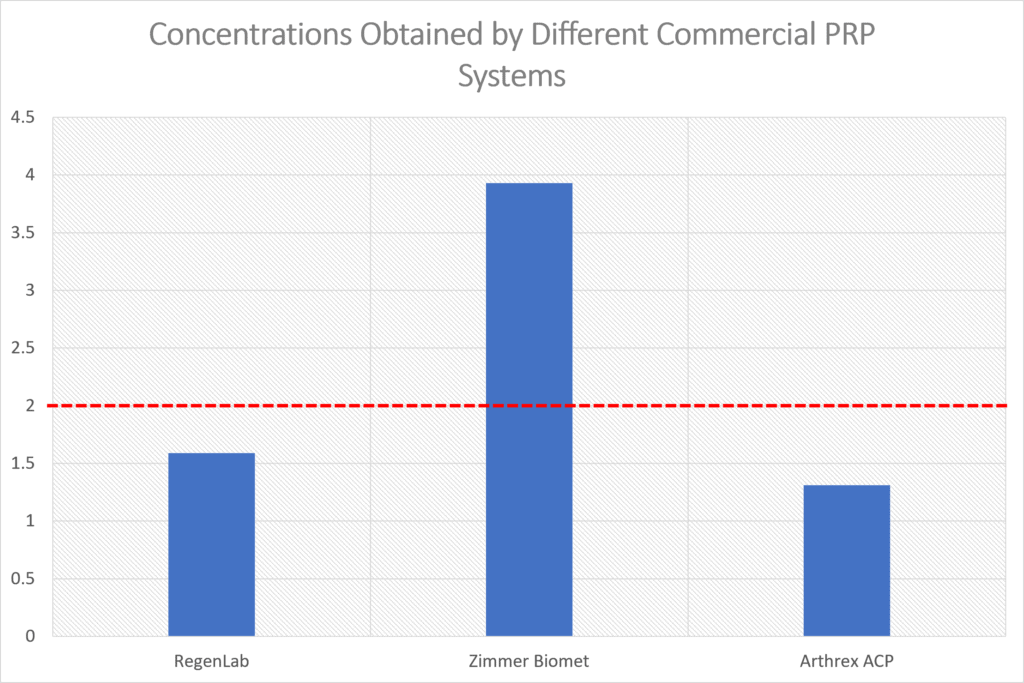
You can see in my graph above created from the data presented by Magalon et al that two commonly used commercial systems produce what I would call “fake PRP”. The problem here is that RegenLab and Arthrex are some of the most popular PRP systems sold. In fact, because of their familiarity with the brand, Arthrex is commonly used by orthopedic practices. However, neither system actually meets the definition of producing PRP which is shown by the red line above. At Regenexx, we go far above the concentrations that can be obtained by these simple bedside units. We use an onsite lab to get the PRP concentrations in the 7-14 X concentrated range.
The upshot? The Bennell JAMA study is now old news and is now replaced by the largest PRP vs. saline study to date that actually used real and not fake PRP. If you’re trying to get PRP to help your Knee Arthritis, please ask which machine the clinic uses and how concentrated it will be. For our standards, that’s at least 4-7X and for many older patients, we recommend 7-14X (more as the patient age goes up).
_______________________________________________
References:
(1) Bennell KL, Paterson KL, Metcalf BR, Duong V, Eyles J, Kasza J, Wang Y, Cicuttini F, Buchbinder R, Forbes A, Harris A, Yu SP, Connell D, Linklater J, Wang BH, Oo WM, Hunter DJ. Effect of Intra-articular Platelet-Rich Plasma vs Placebo Injection on Pain and Medial Tibial Cartilage Volume in Patients With Knee Osteoarthritis: The RESTORE Randomized Clinical Trial. JAMA. 2021 Nov 23;326(20):2021-2030. doi: 10.1001/jama.2021.19415. PMID: 34812863; PMCID: PMC8611484.
(2) Chu J, Duan W, Yu Z, Tao T, Xu J, Ma Q, Zhao L, Guo JJ. Intra-articular injections of platelet-rich plasma decrease pain and improve functional outcomes than sham saline in patients with knee osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2022 Feb 6. doi: 10.1007/s00167-022-06887-7. Epub ahead of print. PMID: 35124707.
(3) Magalon J, Bausset O, Serratrice N, Giraudo L, Aboudou H, Veran J, Magalon G, Dignat-Georges F, Sabatier F. Characterization and comparison of 5 platelet-rich plasma preparations in a single-donor model. Arthroscopy. 2014 May;30(5):629-38. doi: 10.1016/j.arthro.2014.02.020. PMID: 24725317.
(4) Louis ML, Magalon J, Jouve E, Bornet CE, Mattei JC, Chagnaud C, Rochwerger A, Veran J, Sabatier F. Growth Factors Levels Determine Efficacy of Platelets Rich Plasma Injection in Knee Osteoarthritis: A Randomized Double Blind Noninferiority Trial Compared With Viscosupplementation. Arthroscopy. 2018 May;34(5):1530-1540.e2. doi: 10.1016/j.arthro.2017.11.035. Epub 2018 Feb 1. PMID: 29366744.
Original Article: https://regenexx.com/blog/new-day-new-large-prp-saline-control-study-a-comparison-to-bennell-et-al/

.png)








Comments
Post a Comment