The Science Behind Intermittent Fasting and Time-Restricted Eating (TRE) (2026)
Time-restricted eating is just what it sounds like. It's a form of intermittent fasting where you eat all of your meals for the day within a restricted window of time, ranging from two to eight hours. That means you're avoiding food (fasting) for 16 to 22 consecutive hours. Eating within a four- to six-hour window is likely close to metabolic ideal for most. As noted in the paper "A Time to Fast," published in the November 2018 issue of Science:
"Adjustment of meal size and frequency have emerged as powerful tools to ameliorate and postpone the onset of disease and delay aging, whereas periods of fasting, with or without energy intake, can have profound health benefits.
The underlying physiological processes involve periodic shifts of metabolic fuel sources, promotion of repair mechanisms, and the optimization of energy utilization for cellular and organismal health …
In general, both prolonged reduction in daily caloric intake and periodic fasting cycles have the power to delay the onset of disease and increase longevity."

When you eat throughout the day and never skip a meal your body adapts to burning sugar as its primary fuel, resulting in the downregulation of enzymes that utilize and burn stored fat.(1,2)
As a result, you become progressively more insulin resistant and start gaining weight. Efforts to lose weight also become ineffective for this very reason, since to lose body fat, your body must first be able to actually burn fat.
Many biological repair and rejuvenation processes also take place while you're fasting, and this is another reason why all-day grazing triggers diseases while fasting prevents them.
Dr Jason Fung's Story
Dr Jason Fung, in his book entitled “The Complete Guide to Fasting”, articulated the following:
I grew up in Toronto, Canada, and studied biochemistry at the University of Toronto, where I also completed medical school and my residency in internal medicine. After my residency, I chose to study nephrology (kidney disease) at the University of California, Los Angeles, mostly at Cedars-Sinai Medical Center and West Los Angeles VA Medical Centers (then known as the VA Wadsworth). Each field of internal medicine draws its own personalities, and nephrology has the reputation of being a “thinker’s specialty.” Kidney disease involves intricate fluid and electrolyte problems, and I enjoy these puzzles. In 2001 I returned to Toronto to start my career as a nephrologist.Fat-Burning Capacity Is Required for Weight Loss
As just mentioned, to shed body fat, your body must have the ability to burn fat for fuel. While it may seem like this ability should be inherent in everyone, all the time (since we know fat can be used as fuel), metabolic dysfunction triggered by an inappropriate diet and feeding schedule can prevent this. In a nutshell, to be an efficient fat-burner, you need to:- Eat a diet with a higher fat-to-sugar ratio (i.e., more healthy fats and less net carbohydrates), and
- Restrict the timing of your meals so that you're fasting for a greater number of hours than you're eating
While either of these strategies alone (fasting or eating a ketogenic diet) will shift your body from carb-burning to fat-burning, doing them together will yield the fastest results. To learn more about this, see "Why Intermittent Fasting Is More Effective Combined With Ketogenic Diet."
How Time-Restricted Feeding Promotes Weight Loss
So, what's the evidence that time-restricted eating actually promotes weight loss? Aside from a number of animal studies,4 consider the following research,5 published in the July 2019 issue of Obesity.
This study was founded on the premise that by eating earlier in the daytime, you properly align with the natural fluctuations in the circadian rhythm that regulates your metabolism. As a result, weight loss is enhanced.
The question it sought to answer was whether this benefit is mediated through increased energy expenditure or simply lower energy intake. To find out, 11 overweight participants first adhered to an early time-restricted eating schedule, eating all meals between 8 a.m. and 2 p.m. for four days.
For the next four days, they ate all meals between 8 a.m. and 8 p.m. They were also required to maintain a regular sleep schedule throughout. On the last day of each trial, energy expenditure and substrate oxidation levels were measured.
Results revealed meal-timing primarily facilitates weight loss by reducing appetite and increasing fat oxidation. Energy expenditure remained unaffected. As explained by lead author Courtney Peterson, Ph.D., associate professor of nutrition sciences at the University of Alabama at Birmingham:6
"We think the longer daily fast gives people's bodies more time each day to dip into their fat reserves and burn fat. The body is typically maximally efficient at burning fat when people fast for at least 12-24 hours at a time."Overall, eating all meals earlier in the day, between 8 a.m. and 2 p.m., resulted in greater metabolic flexibility, lower ghrelin (known as the hunger hormone) levels, reduced hunger and increased sense of fullness, and this is thought to drive the weight loss.
TRE Improves Weight Loss in Obese Adults
Another study7 published in the Nutrition and Healthy Aging journal in 2018 examined how TRE — without counting calories — affects weight in obese adults. Here, they used an eight-hour restricted eating window.
Twenty-three overweight adults were instructed to eat however much food they wanted between 10 a.m. and 6 p.m. for 12 weeks. For the remainder of the day and night, they were only allowed water. Weight loss and metabolic parameters were compared to the historical records of a group of matched controls.
At the end of 12 weeks, body weight decreased by an average of 2.6% and energy intake decreased by 341 calories per day compared to controls. Systolic blood pressure also decreased by an average of 7 mm Hg.
According to the authors, their findings "suggest that 8-hour time restricted feeding produces mild caloric restriction and weight loss, without calorie counting. It may also offer clinical benefits by reducing blood pressure."
How Restricted Feeding Affects Fat and Muscle in Fit Adults
Overweight individuals are not the only ones who stand to benefit from time-restricted feeding, as evidenced by a 2016 study8 in the Journal of Translational Medicine, which evaluated the effects of TRE on basal metabolism, strength, body composition, inflammation levels and cardiovascular risk factors in fit men. As explained by the authors:9
"Thirty-four resistance-trained males were randomly assigned to time-restricted feeding (TRF) or normal diet group (ND). TRF subjects consumed 100% of their energy needs in an 8-h period of time each day, with their caloric intake divided into three meals consumed at 1 p.m., 4 p.m., and 8 p.m.The remaining 16 h per 24-h period made up the fasting period. Subjects in the ND group consumed 100% of their energy needs divided into three meals consumed at 8 a.m., 1 p.m., and 8 p.m. Groups were matched for kilocalories consumed and macronutrient distribution."
Strength training consisted of a split routine with three weekly sessions on nonconsecutive days for eight weeks. All participants had engaged in continuous resistance training for at least five years before the study.10
Compared to controls, at the end of the eight-week study, the treatment group experienced a decrease in fat mass while maintaining muscle mass and maximal strength.11
Interestingly, while blood glucose and insulin decreased significantly, as expected, so did testosterone and insulin-like growth factor 1, two anabolic hormones.12 Unfortunately, no hypothesis is presented for these findings.
They also found that, aside from a reduction in triglycerides, the time-restricted feeding protocol did "not confirm previous research suggesting a positive effect of [intermittent fasting] on blood lipid profiles."
The researchers address this in the discussion section of the study, postulating that this may be related to the fact that all of the subjects were "normolipemic athletes," meaning their blood lipid profiles were normal to start with. Despite that, the authors conclude:
"Our results suggest that an intermittent fasting program in which all calories are consumed in an 8-h window each day, in conjunction with resistance training, could improve some health-related biomarkers, decrease fat mass, and maintain muscle mass in resistance-trained males."A similar study13 published in the European Journal of Sport Science found that men who performed resistance training for eight weeks while eating all meals within four hours on non-workout days (four days a week) lowered their calorie intake while still increasing strength and muscular endurance.
The Many Health Benefits of Intermittent Fasting: More Evidence
Prof. Satchidananda Panda, has published another study on Jan. 3, 2023. The scientists observed two groups of mice given the same diet, with one given free access to food, while the other was restricted to eating within a feeding window of nine hours each day.“By changing the timing of food, we were able to change the gene expression not just in the gut or in the liver, but also in thousands of genes in the brain,...Our results open the door for looking more closely at how this nutritional intervention activates genes involved in specific diseases, such as cancer.” Panda said.
Nearly 40 percent of genes in the adrenal gland, hypothalamus, and pancreas—key organs for regulating hormones—were affected by fasting. These results suggest that fasting may help manage many diseases from diabetes to stress disorders, with or without pharmaceutical intervention.
Fifty-five percent of these people experienced diabetes remission, stopped their medication, and maintained it for at least one year.
- According to research presented at the Endocrine Society's annual meeting, March 23, 2019, intermittent fasting drastically reduces a woman's risk of breast cancer.
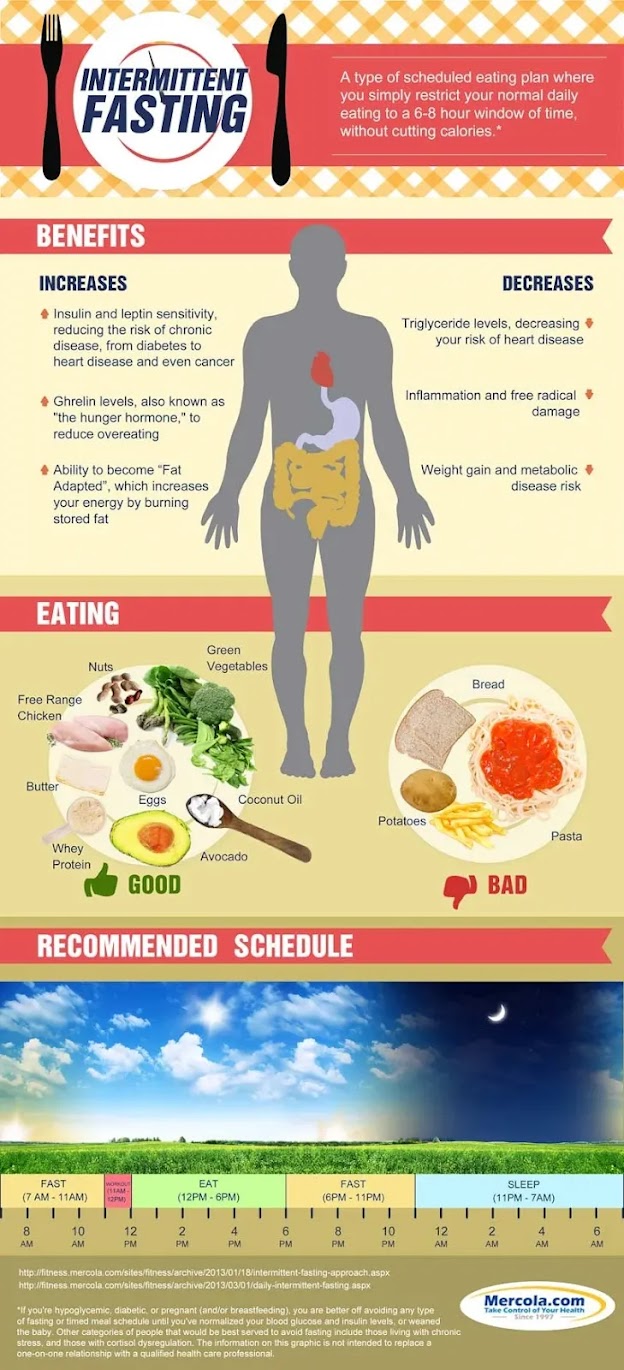
- Promote insulin sensitivity (15,16), which is crucial for your health as insulin resistance or poor insulin sensitivity contributes to nearly all chronic diseases
- Improve leptin sensitivity (17)
- Improve blood sugar management by increasing insulin-mediated glucose uptake rates18
- Lower triglyceride levels (19)
- Increase human growth hormone production (HGH) — Commonly referred to as "the fitness hormone," HGH plays an important role in maintaining health, fitness and longevity, including promotion of muscle growth, and boosting fat loss by revving up your metabolism.
- Research (20,21) shows fasting can raise HGH by as much as 1,300% in women and 2,000% in men. The fact that it helps build muscle while simultaneously promoting fat loss explains why HGH helps you lose weight without sacrificing muscle mass, and why even athletes can benefit from intermittent fasting
- Suppress inflammation and reduce oxidative damage
- Promote multisystem regeneration (22) by upregulating autophagy and mitophagy,23 natural cleansing processes necessary for optimal cellular renewal and function, and promoting regeneration of stem cells (24)
- Prevent or reverse Type 2 diabetes, as well as slow its progression
- Improve immune function by regenerating damaged stem cells (25,26)
- Lower blood pressure (27,28)
- Reduce your risk of heart disease (29)
- Boost mitochondrial energy efficiency and biogenesis (30)
- Reduce your risk of cancer, in part by optimizing autophagy (31)
- Increase longevity (32,33,34) — There are a number of mechanisms contributing to this effect. Normalizing insulin sensitivity is a major one, but fasting also inhibits the mTOR pathway,35 which plays an important part in driving the aging process
- Regenerate the pancreas36 and improve pancreatic function
- Improve cognitive function and protect against neurological diseases (such as dementia, Alzheimer’s disease (37) and Parkinson’s disease (38,39) thanks to the production of ketone bodies (40) (byproducts of fatty acid breakdown, which are a healthy and preferred fuel for your brain) and brain-derived neurotrophic factor (41) (BDNF, which activates brain stem cells to convert into new neurons, and triggers numerous other chemicals that promote neural health).
- Animal research (42) also shows intermittent fasting increases neurons resistance to excitotoxic stress.
- Eliminate sugar cravings as your body adapts to burning fat instead of sugar.
TRE Is Beneficial for Most
Contrary to longer fasts and calorie restriction, TRE is a strategy that can work for most people. Remember, you're not actually limiting or counting calories — you can (theoretically) eat whatever you want in any amount — you're simply restricting the time in which you eat all this food, although you will get better results by eating healthy non-processed foods and not consuming excessive carbs.Weakness and lethargy, which are signs of undernourishment, should not occur. It's a practice that should make you feel good and actually reduce your hunger over time.
Your hunger and craving for sugar will slowly dissipate as your body starts burning fat as its primary fuel. Once your body has successfully shifted into fat burning mode, it will be easier for you to fast for as long as 22 hours and still feel satiated. I typically fast for at least 18 hours a day and sometimes as much as 22 hours.
While time-restricted feeding and intermittent fasting will in theory work regardless of your diet, I do not recommend it if you're eating a preponderance of processed foods. The quality of your diet is particularly important if you're looking for more than mere weight loss.
It's critical to avoid refined carbohydrates, sugar/fructose and grains. Focus your diet on vegetable carbohydrates, healthy protein in moderate amounts, and healthy fats such as butter, eggs, avocado, coconut oil, olive oil and raw nuts.
FMD (Fasting Mimicking Diet) vs Intermittent Fasting (16:8)?
Intermittent fasting (16:8) does not produce sustained autophagy or meaningful IGF-1 reduction at the level required for the longevity benefits seen with FMD. The 5:2 diet (2 days of ~500 kcal restriction per week) shares some metabolic overlap but uses a different macronutrient composition and does not match the FMD’s specific nutrient-sensing suppression formula. FMD is a distinct, more intensive protocol with a separate evidence base.Time-Restricted Eating vs Calorie Restriction in Weight Loss - NEJM (April 2022)
This randomized clinical study concluded that among patients with obesity, a regimen of time-restricted eating was not more beneficial with regard to reduction in body weight, body fat, or metabolic risk factors than daily calorie restriction.- 1 Cell February 8, 2018; 172(4): 731-743.E12
- 2 Medical News Today February 8, 2018
- 3 Science November 16, 2018; 362(6416): 770-775, Page 1
- 4 Medical News Today July 4, 2018
- 5 Obesity July 24, 2019; 27(8), Abstract
- 6 Inverse July 24, 2019
- 7, 28 Nutrition and Healthy Aging 2018; 4(4): 345–353, Abstract
- 8 Journal of Translational Medicine 2016; 14: 290
- 9 Journal of Translational Medicine 2016; 14: 290, Abstract Methods
- 10 Journal of Translational Medicine 2016; 14: 290, Methods Training
- 11 Journal of Translational Medicine 2016; 14: 290, Abstract Results
- 12 Journal of Translational Medicine 2016; 14: 290, Results and Discussion
- 13 European Journal of Sport Science 2017; 17(2): 200-207, Abstract
- 14 Science November 16, 2018; 362(6416): 770-775
- 15, 42 PNAS May 13, 2003; 100(10): 6216-6220, Abstract
- 16 Cell Metabolism June 5, 2018; 27(6): 1212-1221.e3
- 17 PLOS ONE 2014; 9(3): e92214
- 18 Journal of Applied Physiology July 28, 2005: 99(6); 2128-2136, Abstract
- 19 Medscape March 7, 2019
- 20 Intermountain Healthcare Press Release April 3, 2011
- 21 Nutrition, Metabolism & Cardiovascular Diseases November 2013; 23(11): 1050-1057
- 22 Cell Metabolism June 2015; 22(1)
- 23, 31 Clinics 2018; 73: e814s
- 24, 25 Cell Stem Cell June 5, 2014; 14(6): 810-823
- 26 USC News June 5, 2014
- 27 Journal of the American Society of Hypertension 2018; 12(1): 42-49 (PDF)
- 29 American Journal of Cardiology 2008 Oct 1;102(7):814-819
- 30 Frontiers in Physiology May 3, 2019, Caloric Restriction, Intermittent Fasting, and Mitochondrial Function
- 32 NIH.gov Press Release September 6, 2018
- 33 The Harvard Gazette November 3, 2017
- 34 Journals of Gerontology, Series A July 17, 2015; 70(9): 1097-1104
- 35 Aging 2018 Jul; 10(7): 1640–1648
- 36 Cell February 23, 2017; 168(5): 775-788
- 37 Neurobiology of Disease April 2007; 26(1): 212-220
- 38 Aging Research Reviews August 2006; 5(3): 332-353
- 39 Washington Post December 31, 2012
- 40 IUMB Life 2017; 69.5 DOI: 10.1002/iub.1627, Conclusion
- 41 Annual Review of Nutrition 2005;25:237-60


.png)







Comments
Post a Comment